Abstract
Aging: no one wants to, but everyone does. Many people are scared of aging mostly because they think of ending up in a bed, doing nothing other than staring at the ceiling and depending on other people who have to sacrifice their free time and strength to care for them. Under these circumstances, not only is the quality of life gone, but also the relationship with relatives can suffer because someone might become a burden.
Scared about this fate, the elderly (and disabled) sometimes wish for suicide or euthanasia. Many need help if their independence is affected because of advanced age. Additionally, euthanasia is illegal in most modern countries.
Aging: no one wants to, but everyone does. Many people are scared of aging mostly because they think of ending up in a bed, doing nothing other than staring at the ceiling and depending on other people who have to sacrifice their free time and strength to care for them. Under these circumstances, not only is the quality of life gone, but also the relationship with relatives can suffer because someone might become a burden.
Scared about this fate, the elderly (and disabled) sometimes wish for suicide or euthanasia. Many need help if their independence is affected because of advanced age. Additionally, euthanasia is illegal in most modern countries.
A new area of research called Ambient (or also Active) Assisted Living (AAL) exists and addresses these concerns. The first ideas in AAL research were introduced in the 1970s, which included technology use from several fields (e.g., robotic solutions). Figure 1.1 shows the first sketches of how such systems could look at that time. Some of these concepts, which were developed and funded by the Japanese Society for the Promotion of Science in 1985, are summarized in [1].
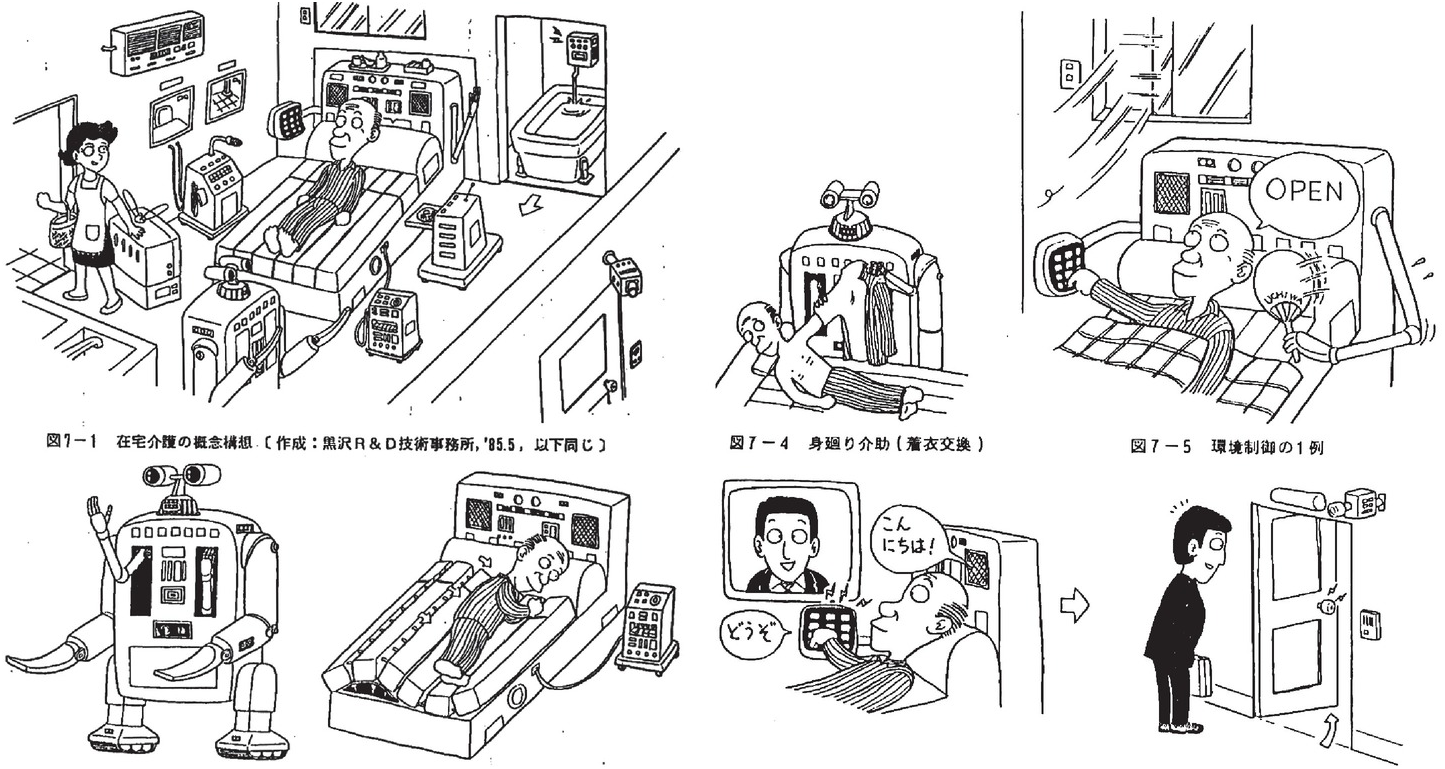
Figure 1.1 The first vision of AAL as developed in Japan 40 years ago[1]. It is a life support system for the elderly. Japan Society for the Promotion of Science. 1985–86.
Aging is an unavoidable and natural process. Physicians have investigated whether there is a possibility of slowing down the aging process, but aging is a multifactorial process and cannot easily be manipulated by simple behavioral rules [2]. According to [2], proper nutrition intake, physical activity, and avoidance of obesity and smoking allows for healthy aging and a high quality of life for as long as possible. Antioxidants and caloric restriction promise to positively manipulate the aging process; however, no study has proven any reliable effect. Additionally, there is also a risk of harming the human body by restorative interventions in the aging process, e.g., by caloric restriction [2].
Why do living beings age? According to [2], the aging process is not programmed in the genes of a being, it is more of an evolutionarily successful strategy, which is the outcome of the extrinsic death risk (i.e., the risk of getting killed by accidents or enemies), making it useful to limit the amount of resources for preserving and repairing capabilities.
Sooner or later aging leads to death, and death frees up the bounded biological resources (the different bases, amino acids, proteins, etc.), which supports the development of new life. New life can try to perform better, as explained by Charles Darwin’s theory of evolution by natural selection [3]. While physicians and biologists try to find a method that avoids or at least slows down the aging process, engineers work on technological solutions to maintain the independence of the elderly.
In this volume, current AAL needs and technology are presented to give an outlook on current developments entering the market and research forming the future. This chapter introduces the reader to the background of AAL and its link to robotics.
1.1 Technological Development
This new research field of AAL is therefore a multidisciplinary field connecting researchers from several disciplines (physicians, social researchers, engineers, etc.) to help patients keep their independence. However, aging itself is not the enemy of this research area. Aging leads to multimorbidity [2], which means that the older someone gets, the more fragile the person becomes. Consequently, AAL technology deals with preventing age-related diseases and their secondary diseases or complications (which includes young people) and assisting disabled people, especially regarding age-related diseases. Many wearables and apps have entered the market, mostly using devices like smartphones, which try to support the user in a healthy lifestyle, e.g., apps for weight loss [4], glycosometers, which are add-ons for smartphones [5], etc. Wearables have been used since the first astronauts’ flight to space. For example, in space suits during extra-vehicular activities (EVA), according to [6], plethysmographs (for breath detection, as well as lung analysis), Galvanic Skin Resistance (GSR) sensors (for stress detection, e.g., by sweating), skin temperature sensors, and pulse oximeter sensors (for heart rate and oxygen saturation of the blood) were used to check the health status of the astronauts.
However, the technology has now reached a limit, thus allowing researchers to go a step further; instead of just developing new measurement and intervention devices, apartments and buildings can be equipped with sensors and devices that support the user when needed. The apartments and houses become a kind of assistive robot: omnipresent in the environment, but unobtrusively implemented to avoid the feeling of permanent screening. According to [7], researchers working in the AAL field have, in recent years, developed new technological solutions based on ambient intelligence. Ambient intelligence is aiming to empower new capabilities through a digital environment and at the same time being sensitive and adaptive to a user’s needs. AAL is not only potentially able to prevent, cure, and improve wellness and health conditions of users, but it also improves safety conditions, e.g., by fall detection, emergency alerts, video surveillance systems, etc. [8]. Also, support in activities of daily living (ADL), e.g., by mobility support and automation, belongs to the field of AAL [9]. Furthermore, communication technology belongs to this field too, as the elderly can connect and communicate more easily with friends and relatives [10]. On the other side, mobile and wearable sensors are more focused on health-related sensor technology, e.g., glucometers, blood pressure devices, and cardiac activities [7]. The idea that robots belong to the field of AAL has already been proven by several research groups, e.g., [11], [12], and [13], aimed to assist movement reduction, fetch objects [14], or transfer support e.g., from bed to wheelchair [15]. According to [7], the smart home is one topic belonging to the AAL sector. Here the analysis and fusion of different types of sensor data helps in obtaining and analyzing information to automate several tasks as well as to increase comfort [16]. Following this approach, modern AAL projects consider not only sensors and devices for automation and comfort, but also the fusing of wearables with smart homes. The entire apartment can be automated, resulting in a robotic apartment. This scenario can be seen as the ultimate fusion of smart homes, wearables, and robotics. More details about such projects are described in Chapter 5.
1.2 Social Development
Why has AAL become so important? The importance of AAL is related to demographic changes, which did not start yesterday. Indeed, the societal demographic changes felt today started at the beginning of the nineteenth century with a growing world population [17].
Technological and (especially) medical knowledge was worse in the nineteenth century than to today. By continued improvements in the medical field, many medications (e.g., arsphenamine [18], and later on penicillin) which allowed for curing deadly diseases, e.g., syphilis [19], have been found. Additionally, when compared to the time before the nineteenth century, child mortality also dramatically changed. For example, the composer Leopold Mozart and his wife Constanze Weber were parents of Maria-Anna Mozart and Wolfgang Amadeus Mozart (see Figure 1.2), as well as of five other children who didn’t live beyond 16 years of age. High child mortality was normal. Also, age-related population distribution, as depicted in Figure 1.3, was comparable to a triangle. Families were large and lived together for longer; there was always the possibility that children would take care of their senior parents. Following improved medication, families started to change because normally children are expensive to take care of. Large families became impoverished because of too many children.


Later on, careers became more important. Parents could earn money and consequently grant one or two children a better life. This led to the fact that children would leave the extended family home and become busy with their own smaller nuclear family. Parents and grandparents normally live in rural areas owing to low living costs, whereas their children move to large cities to work and have better career chances [21]. Therefore, cities like Munich, Hamburg, and Frankfurt [22], become younger, whereas the overall population of industrialized nations is aging.
Figure 1.4 shows the current and future related population distributions. It is clear that the number of young people who can care for the elderly (as compared to Figure 1.3) is extremely reduced, and the situation is projected to worsen.


Figure 1.4 Left: Age structure of the population in Germany, December 2013. Right: The expected age structure of the population in Germany, December 2060, compared with 2013.
Caregiver careers are not very highly appreciated by the young population. In Western Europe, poor refugees often work in care homes. However, most care homes now have difficulties in acquiring adequate staff, and the care costs are increasing at the same time. The demographic change is not only a European problem; all industrialized nations are facing the same issue. In Japan and China, the demographic change has an even larger impact. Therefore, many AAL robots and products are already trying to enter the Japanese market (see Section 3.6). To solve the care problem, AAL products have to help elderly patients increase their independence.
1.3 History of Mechatronic/Robotic Environments
It is not surprising that technology is one key to solving the problems caused by demographic change. However, robotics can seem frightening to the elderly, since many do not have a very high affinity for technology. Robots, especially those that resemble humans (also called humanoids) are from a specific point a deterrent for people, especially the elderly [23]. But this perception will change once the next generation needs AAL technology. Additionally, in European stories, robots are normally depicted as evil; e.g., according to [24], movies such as The Terminator [25] and The Animatrix [26] prove this theory. In Japan, robots have more positive role in literature and film, or at least the “evil” or “bad” roles are more equally distributed between humans and robots [24]. Modern literature and movies, which influence the relationship between people and robots, predict that robots will be accepted in future households. Already some devices prove useful at home, e.g., as vacuum cleaners [27].
In this respect, Japan is more advanced than Europe in two ways: first, Japan is suffering more from demographic change, as already mentioned in Section 1.2, and second, Japan has a very old history in the development of robots, e.g., in form of Karakuri.
According to [28], the first Karakuris was described in the Konjaku Monogatari in 1110; it is written that a Karakuri was prepared to supply the farmers in a field (during a drought) with water. Further documents, which prove the early development of robots in the form of Karakuris, can be found in a three-volume book Karakuri Zui, written by Hanzō Yorinao in 1796. Compared to the robots later developed in Europe, Karakuri were completely developed out of wood, instead of metal, iron, and screws. Karakuri were also able to express emotion through specialized head movements. Karakuri robots had different abilities, e.g., shooting up to five arrows, when after the fifth arrow the Karakuri express disappointment because of missing the aim (Yumi Karakuri); serving tea (Chahakobi); acrobatics; and stilt walking controlled by a device with rods and strings (Sashigane).
These first robots did not work with electricity or digital processors as those of today. Their technology was strictly mechanical, on the level of developing a clock. Ōno Benkichi (physician and mathematics, 1801–1870) and Tanaka Hisashige (also called Karakuri Giemon, 1799–1881) developed the famous Mannen-Tokei clock. This Japanese clock (see Figure 1.5) adjusted the hours to differing day/night lengths of winter and summer time by asymmetric tooth wheels in the clockwork. The clock adjusted its length mechanically by sliding on the upper half of the clock face or dial six hours before and after noon or midnight. Thus, the mechanics adjusted to the need of the user, which is the same principle applied for the Toyota production system (TPS), which adjusts to need of the worker, and for Japanese cooperative robots since the 1990s. We use a similar approach for our robotic ambience notion described in this volume.

Figure 1.5 Japanese pillar clock, 1800–1870; The “pillar” clock is a type peculiar to Japan, in which the driving weight itself is the time indicator as it falls slowly past a scale of hours mounted below the timekeeping part of the movement. The hour numerals are adjustable by hand to allow for the varying hours of the day and night through the year. The Japanese system of “temporal hours” timekeeping until 1870 divided the day and night each into six equal “hours.” The length of these “hours” differed throughout the year as the seasons changed.
It can be said that all these technologies can adjust to human activity and the environment. In that sense, the Japanese clock system (Figure 1.5) is adapted to the difference of sun light hours in summer and winter.
For example, to control the chahakobi Karakuri robot, which is serving tea, the host and the guest have to define the starting and ending points of the movements together. The Karakuri robots are using potential energy, stored in an updraw coil spring, which will be transformed into kinetic energy. Additionally, the feet of the robot pretend to walk. The complex mechanism is triggered by a plate in the hands of the chahakobi Karakuri robot, where the teacup is placed. These very first pressure sensors enabled the users to trigger when the robot shall move 180° around and go back.
Therefore, Karakuri robots include the user (or guest) in their show and put the guest at the center of the attention, which can (and should) easily laugh by the mistakes of the Karakuri robot. The life expectancy of the Karakuri is between 50 and 100 years, and their modular construction allows for easy repair by disassembling. All these aspects have the psychological success that in Japan robots are not a threat to the population. Therefore, the Japanese philosophy of Kaizen (which means continuous improvement) fused with the Karakuri create the philosophy of Karakuri-Kaizen, the basis for a sustainable and a highly efficient production process in modern factories of Japan.
This functional principal of Karakuri is especially visible in construction areas. On high-rise construction sites, the devices used are very similar to the Karakuri principal; their rotation, lifting, and rope mechanisms are partly automated. The only difference here is that these devices are digitally controlled.
At the end of the 1970s, the Shimizu Company started to experiment with construction robots. Computer-controlled CNC processes for Japanese timber engineering has existed since the 1960s. The Sashigane control from the Karakuri, which has been available since the 1700s in Kabuki Theatre (during the Edo period), is the basis for the Sakauchi method used in Japan (see Figure 1.6).

Left: Sashigane lifting press.

Right: Karasu Tengu-mechanical puppet.
The Karakuri principle is also found in buildings in different occurrences, e.g., the Zashiki Karakuri, a small device for the reception room (mostly only for private use), or the Yashiki Karakuri or Ninja Yashiki, where the whole house is equipped with manipulability mechanisms (Figure 1.10). Therefore, in houses from the Mochizuki Izumonokami, in Kōka at Kyōto, from 1487, different specialties like hidden subfloors, folding ladders, double walls, etc., are implemented. Most famous are the rotating walls (donden gaeshi), which are access points to hidden rooms and floors, or cavities to hide weapons (yukashita mono kakushi), flush doors (kakushido), etc. This approach could be named Karakuri-Architecture, Apartment-Karakuri, or Building-Karakuri, which means to unobtrusively embed different mechanisms into the environment, a similar approach to the AAL technology of the future (more details can be found in Section 2.2). A good example of the integration of devices is the Kouka-ninjya house in Kōka [29], which was a former inn for feudal lords or ninjas. Here, many “secret” devices for hiding can be found if the situation required an escape (see Figure 1.7).


The Karakuri technology has also influenced Europe, e.g., use of the rotating stage in theater during the Edo epoch (1602–1868) was used in the Kabuki Theater play “Nakamura Denshichi.” Furthermore, the prototype of the modern rotating stage has been used by Namiki Shoza (1730–1773) in the theater play “Sanjikoku Yofune no hajimari” at the Za-Kabuik-Theater in Ōsaka in 1758. The rotating stage, which found its perfection in 1848, had two opposite rotating stages, and was introduced in Europe at the end of the nineteenth century. By using the Karakuri mechanism, whole stage sets can arise in seconds, which allows the whole stage to work as a Karakuri mechanism, proving once more the success of unobtrusive implementation of complex technology into the environment. The invention was named as “mawari-butai” (see Figure 1.8) and there are still some that are performing as the Eirakukan in Izushi [30]. Even today this is inspiring latest research projects, which try to develop robotic rooms by implementing high tech robotic devices and sensors unobtrusively into the environment [31] (see also Chapter 5).


In Europe, the modern history of automats probably starts with Jacques de Vacaunson when he invented a mechanic flute-playing device that blew air through a real flute (see Figure 1.9) [32] [33].

The modern crewed spacecraft (Figure 1.10) can be considered a modern version of the Nijo Jinya building [29], where mechanical devices are integrated on the interior living environment. The astronauts can operate with these machines and devices for everyday living and to accomplish their work.



Finally, we can find the new modern version of the Karakuri concept in the transformer toys developed and commercialized by the Japanese company Bandai [34].