Abstract
In this chapter, several projects will be presented in order to show the current state of the art in the research and development of the integration of ambient integrated robotics. The projects focus especially on the support of the elderly and fragile people. The main aim of each single project is to keep the user physically and mentally active in order to slow down the process of senility. All the tasks that the user cannot do alone anymore must be supported by the technology. Here however, the main difficulty in each presented project is to establish the system in a way that only the minimal necessary support is offered, otherwise the user could become too inactive leading to an accelerated process of senility.
In this chapter, several projects will be presented in order to show the current state of the art in the research and development of the integration of ambient integrated robotics. The projects focus especially on the support of the elderly and fragile people. The main aim of each single project is to keep the user physically and mentally active in order to slow down the process of senility. All the tasks that the user cannot do alone anymore must be supported by the technology. Here however, the main difficulty in each presented project is to establish the system in a way that only the minimal necessary support is offered, otherwise the user could become too inactive leading to an accelerated process of senility.
5.1 Project GEWOS
The objective of GEWOS (Gesund wohnen mit Stil – Healthy Living with Style) was to develop a sociotechnical furniture that animates the elderly to move more actively, in order to enable a healthy lifestyle. By implementing the appropriate technology into an armchair for the living room, this health-support system is unobtrusively integrated into the living environment of the elderly. The overall system consists of motion sensor unobtrusively integrated into the seat, training devices (e.g., rows), a TV (as interface), and some vital measurement devices like pulse oximetry and ECG. By using Wi-Fi, the armchair measurement gets directly connected with a server (via internet). Using a remote controller concludes the overall system integration into a smart living environment, allowing to not only control the TV and display measurement results, but also to control home electronics like light switches.
A specially designed graphical user interface (GUI) allows the elderly an intuitive access to the different service functions offered by the chair. However, the project confirmed the importance of the end-user motivation and design if such systems should be applied in the user’s home environment. In order to enable training and at the same time make the armchair look convenient, rowing oars have been integrated into the chair. The oars are covered by the arm rest, which let the armchair look like a normal armchair. Stand-assist as well as position is also provided, which allows the user to train (guided by the GUI of the GEWOS TV) directly on the chair (see Figure 5.2).
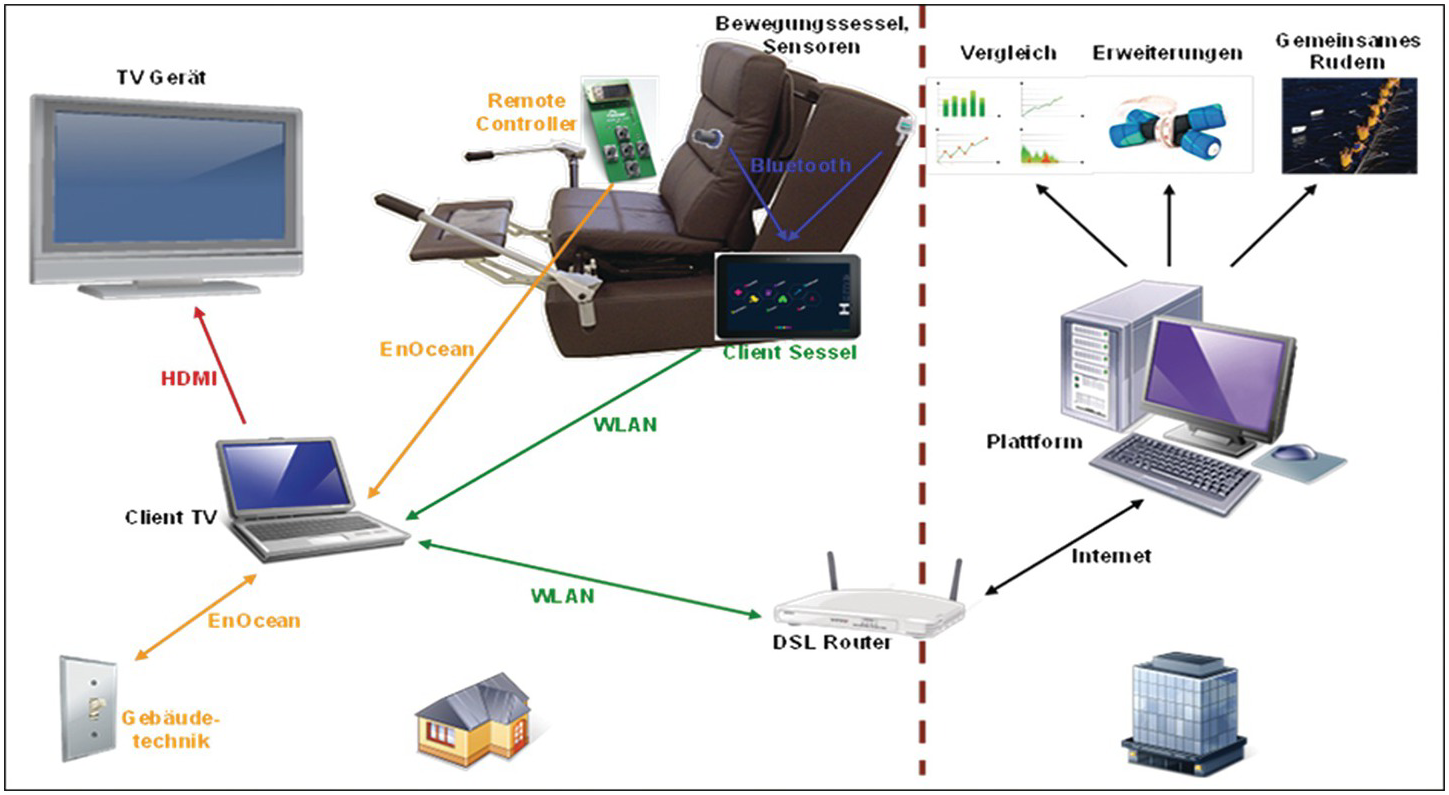
Figure 5.1 The overall system architecture of the GEWOS project.

Figure 5.2 Top left: The GEWOS armchair with unobtrusive AAL technology. Top right: The GEWOS armchair with uncovered rows. Bottom left: Stand-assist. Bottom right: Training guided by the GEWOS GUI.
To motivate the user to train, a video-gaming style has been implemented. As Figure 5.3 demonstrates, the user sees a virtual river, which he can row down, using the implemented oars in the arm rests. While the elderly is just playing a game, he is in fact training guided movements via use of the oars.

5.2 Project LISA
Devices, like those mentioned in Section 5.1, can be expensive to replace an existing furniture. Although this fact does not sound so critical, the elderly do not easily separate from their belongings, because they link them with memories. Therefore, for the AAL research, it is a major topic to develop add-ons, which are also compatible with the given environment.
This is one of the most challenging factors: to develop a technology that can be easily installed in a different and absolutely customized, but not structured, user environment. For example, a more structured environment is the car. If someone wants to install a navigation device into a car, the installation is easier, because of the standardization (in this case the windscreen). In an apartment, this luxury does not exist; even door sizes differ from apartment to apartment. Nevertheless, project LISA’s objective is to find a solution here by developing plug-and-play smart AAL walls. Additionally, the multimorbidity of the elderly must be considered, which leads to complex and highly individual multiple constraints. Therefore, the multidimensionality, i.e., the possibility to operate several modules of the offered assistance at once is of central importance [157].
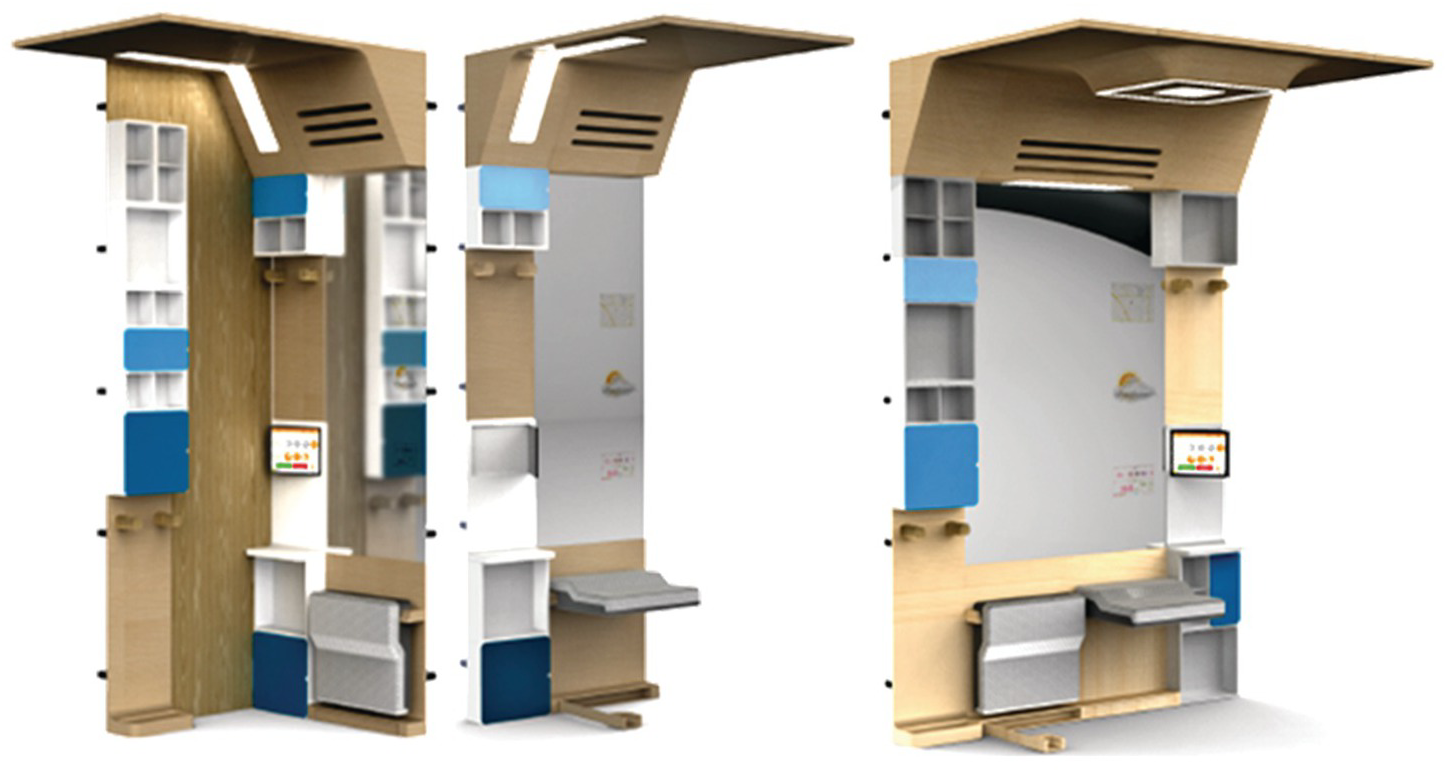
For the very first time, the apartment was structured in their different areas: living room, bed room, kitchen, bath room, and entrance areas (see Figure 5.4).
For each area, a unique solution must be found. To do this, a basic module, which can easily be installed (in a few hours) must be developed. This smart wall device will later on serve as an interface for various modules that offer different services.
Depending on the apartment area, the offered services must distinguish that, e.g., an induction cooker is very useful in the kitchen but makes less sense in the entrance area. According to this new approach, the different apartment areas have been evaluated according to their interface complexity (current, internet, water supply, etc.). The results showed that the entrance area belongs to the most promising areas, according to the high need of the elderly (here the elderly and fragile face a lot of challenges, forgetting keys or choosing the wrong coat for the actual weather condition, which may lead to influenza, etc.) and the least complexity regarding the interface compared to the bathroom and kitchen, which need a water supply interface.
As the next necessary step in this approach, the service functions must be defined. According to the project, investigations following overall functions have been considered (also illustrated in Figure 5.9): light (including color and intensity), remembering function (to avoid that the elderly lose or forget their keys, etc.), shoehorn (to ease dressing), vital measurements (to figure out potential risks of diseases together with the weather report), robotic assistance (to carry the belongings of the user), and a stand-assist (for the case of a weak blood circulation).
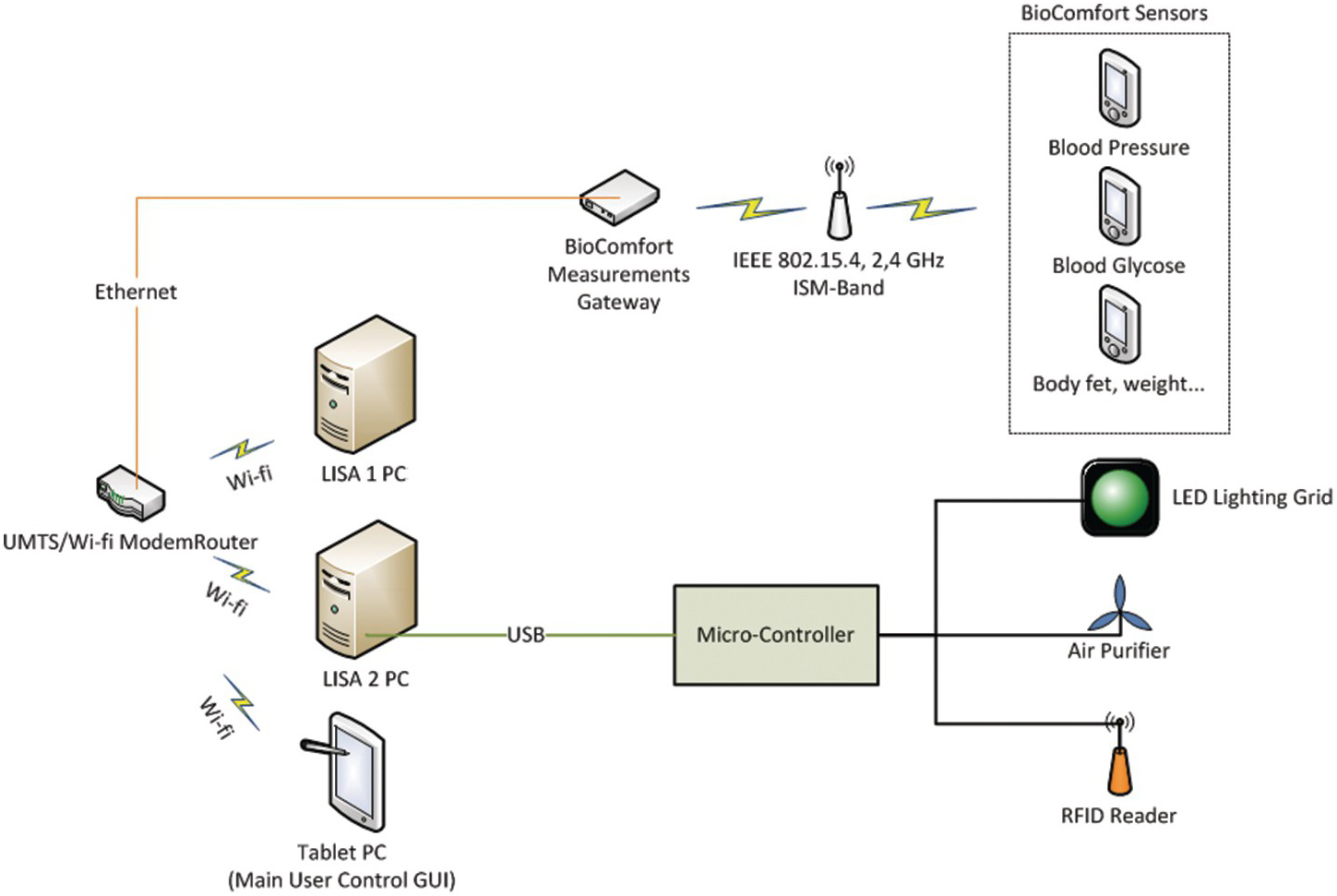
There are some functions already on the market, like the vital measurement, which has been implemented in the terminal. Every household has a blood pressure meter, a scale, or a blood glucose meter. Here, however, the main objective of the project LISA is the seamless integration or interfacing of these existing products. The mentioned devices use a Wi-Fi transmission to send their data to a local server, which is used to store the data, in order to plot them on a user-friendly GUI and to show the health status over time. This allows to more efficiently interpret, e.g., blood pressure, as the measurements work in relation to each other instead of just giving a single result. The overall system architecture is depicted in Figure 5.6, and also shows the communication to the reminding function.

Figure 5.5 Potential service modules for the smart AAL walls. Top left: Light and air purifier. Top middle: Robotic assistance. Top right: RFID Antenna and processing unit with USB interface. Bottom left: Shoehorn for dressing assistance. Bottom middle: Blood pressure meter for health status estimation. Bottom right: Stand-assist.
The reminding function uses RFID technology to identify, by tags, the appropriately marked objects. The tags are passively powered and can be very small, which allows for marking, e.g., the keys unobtrusively. An antenna implemented in each shell of the shelf is able to detect the tag (see Figure 5.5). Using Arduino Micro as the processing unit, it is possible to read out the RFID antenna and to forward the information to the local server, where the availability information of the object is stored. The user can access the information by using the LISA GUI as shown in Figure 5.7. As the Arduino is supplied and interfaced by USB, this function is easy to install by plug-and-play, which means that the modularity aspect is fulfilled.
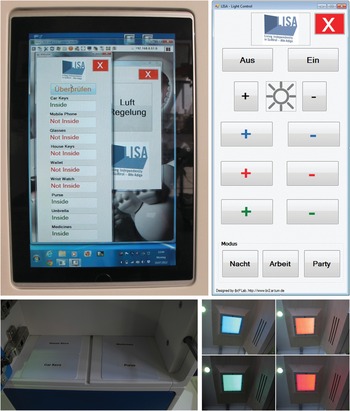
Figure 5.7 Top left: GUI on the touch screen as user interface, showing the result of the RFID tag scan. Bottom left: The test tags in the shelf for demonstration. Top right: An exemplary user interface for setting up the light condition. Bottom right: The different results which can be set up.
The GUI allows the user to also control the function of the light and air conditioner [158]. It also showed that the light color and intensity can directly influence the mood of a senior. Additionally, the potential is given to link the RFID remind function to the light, e.g., when the door is opened, in order to enable a silent (i.e., not stigmatizing) alert, which warns the user not to forget the key in the shelf, before closing the door.
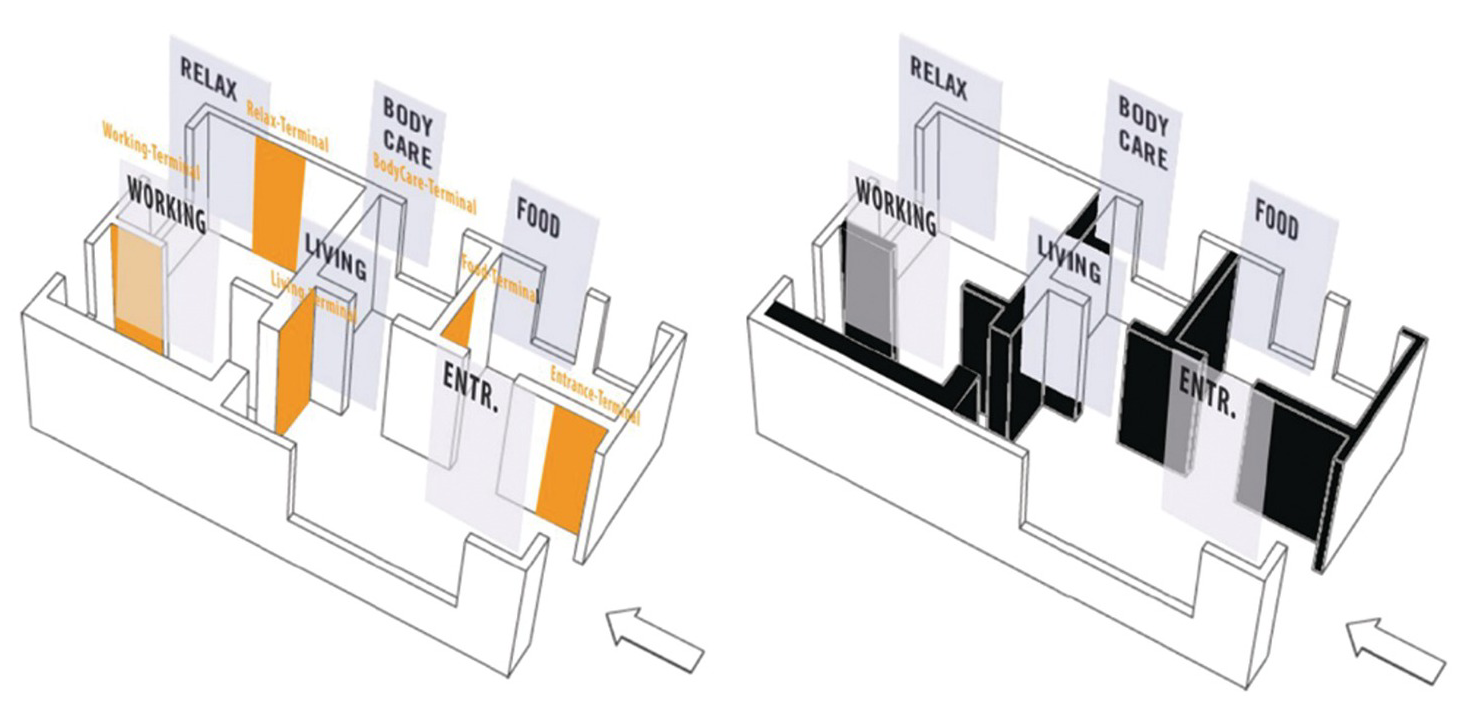
The modularity aspect of the smart AAL wall LISA is not limited to the potential service modules. As part of customization, and considering the different sizes of the apartments, the terminals can be set up as shown in Figure 5.8.
5.3 Project PASSAge
Mobility means life quality, especially in old age. Therefore, it is not surprising that there exists a huge variety of mobility aids (rollator, Stairlift, E-Scooters, etc.). Up to now, however, it is still very challenging for the elderly to take part in the public road traffic. This is mostly because when mobility aids are being developed (or houses, trains, etc.), the interface for these aids are mostly neglected. For example, the rollator is nowadays helping a lot of the elderly to stay mobile. However, there are a lot of entrance doors, which have “just” three steps (because it looks nice). Unfortunately, for someone who is fragile and needs a rollator as support, the three steps are invincible with the rollator.
Here, the PASSAge project aimed to investigate such “mobility gaps” in order to design interfaces on the hard- and software level to develop a seamless mobility chain from the bed to the entire world. The major focus in this section will be on the home environment.
Demographic changes have an impact on the future planning of the mobility for an independent life. Accessibility, according to the existing standards, can only partially solve the problem; therefore, holistic concepts are needed. Distances, which can be done by foot or by bicycle are usually straightforward, but the risk for elderly as pedestrians or cyclists is high. For example, as pedestrians, the risk to die by an accident is increased by 3.8 times. On the other hand, the risk of cyclists getting killed by an accident increases by 5.8 times according to [159].
This is because of age-related reduction of the physical and cognitive competencies among the elderly, which can lead to small mistakes with serious consequences. To secure the mobility of the elderly, existing mobility aids like the rollator should be further developed by add-ons, and additionally taking into account that future seniors will be healthier and more mobile than the current elderly [160]. The objective of the project was to provide a cross-linked and flexible infrastructure for a variety of mobility components, where the different components are not in competition with each other but create synergies by cooperation in order to secure the mobility and agility of the elderly. The smartphone is thought to be an interface for controlling the PASSAge System environment, which could also be used for navigation and health management (using appropriate apps).
Different constellations and connections in the value system offering different optimal solutions are what institutions and companies concentrate on in the development of assistance and aid systems [161]. Four different scenarios (or use cases) were defined in order to estimate the potentially best solutions within PASSAge. The first use case is the AAL-House, including care phones, safety bracelets, video telephony, alarm detectors for smoke water, etc. The second use case considered E-Cars of different sizes, walking aids, rollators, scooters, lift systems, and social services. The third use case described shopping, errands, doctors and hospital visits, culture and church events, visiting friends, and relatives. The fourth use case considered user interfaces, e.g., on smartphones, vital signs measurement (blood pressure, activity profile), navigation, service platforms, etc.
The main focus is set to Use Cases 1 and 2. Especially for the Use Case 1, the indoor support and use of robots has been investigated. Robots are difficult to include into the home environment, because they are mostly large, heavy, and expensive. Therefore, the use of the TurtleBot has been investigated.
The TurtleBot, for robots, is low-cost, lightweight, and small. Its disadvantage is the reduced payload, which leads to the question: how can a robot, which resembles a toy, support the elderly in their activities and mobility? For this purpose, a new interface (using PLE with a 3D printer), which allows the robot to connect to a rollator has been designed as demonstrated in Figure 5.9.

Figure 5.9 The new interface, which allows the TurtleBot to interface with the rollator.
This approach allows the TurtleBot to move the rollator to the user, despite the payload being very low. The main idea behind this development is to ensure that an end user can always reach the rollator by ultra-low-cost robots. However, this idea has the challenge to answer the question: how can a user control this robot?
To investigate the potentially best solution, a special GUI has been designed (shown in Figure 5.10), where the end user could test different controlling options.
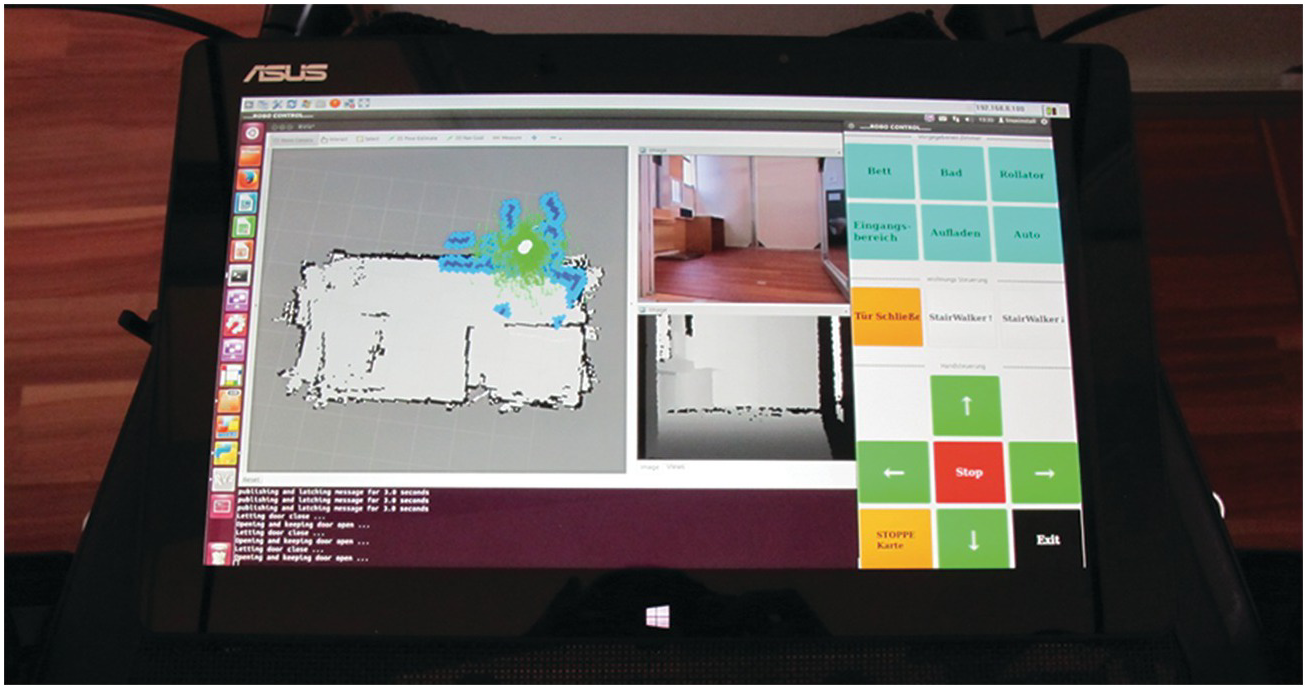
Figure 5.10 User interface, which allows the user to command and navigate the TurtleBot.
The arrow buttons allow the user to directly navigate the robot. A map, showing the location of the robot in the apartment as well as the RGB image (and depth image), gives the user a hint as to where the robot is (in case the robot is hiding in another room). Even though this kind of control is very challenging for the elderly, it always offers the possibility to interfere if the robot is making a mistake.
At the top, predefined tasks, e.g., how to connect to a rollator, are defined. By pressing one of these buttons (using the touch screen of the tablet PC depicted in the window), the robot acts completely independent. Even though this kind of user input is preferred, the accuracy of the navigation of the TurtleBot is just enough to connect with the rollator. If the task needs a higher accuracy, the user must support the TurtleBot by the arrow buttons (Figure 5.1).
Alternative inputs, like gesture control using the Leap motion sensor (as described in Section 5.4), or by voice control, showed a disappointing and weak result. The motion control is not intuitive enough for a mobile platform, whereas voice control fails mostly because of the different pronunciations, which are often influenced by dialects. Additionally, for the elderly, it is difficult to recall specific terms and to understand that they cannot talk to the robot like to a human, at least with current technology.
The alternative to pointing a position directly on the map by using the touchscreen was also not highly appreciated by the end user. However, still more preferred it to arrow buttons; the main critique of the touchscreen was that it is mostly too small to point to the correct position (especially on a smartphone, as shown in Figure 5.11). Combined with the reduced accuracy of the TurtleBot, the navigation of the robot becomes challenging again. Nevertheless, the subjects of the test mainly criticized the interface. As soon as the tester got used to the control option, the feedback was mainly good. This demonstrates the high potential of even such small and cheap robots like the TurtleBot.
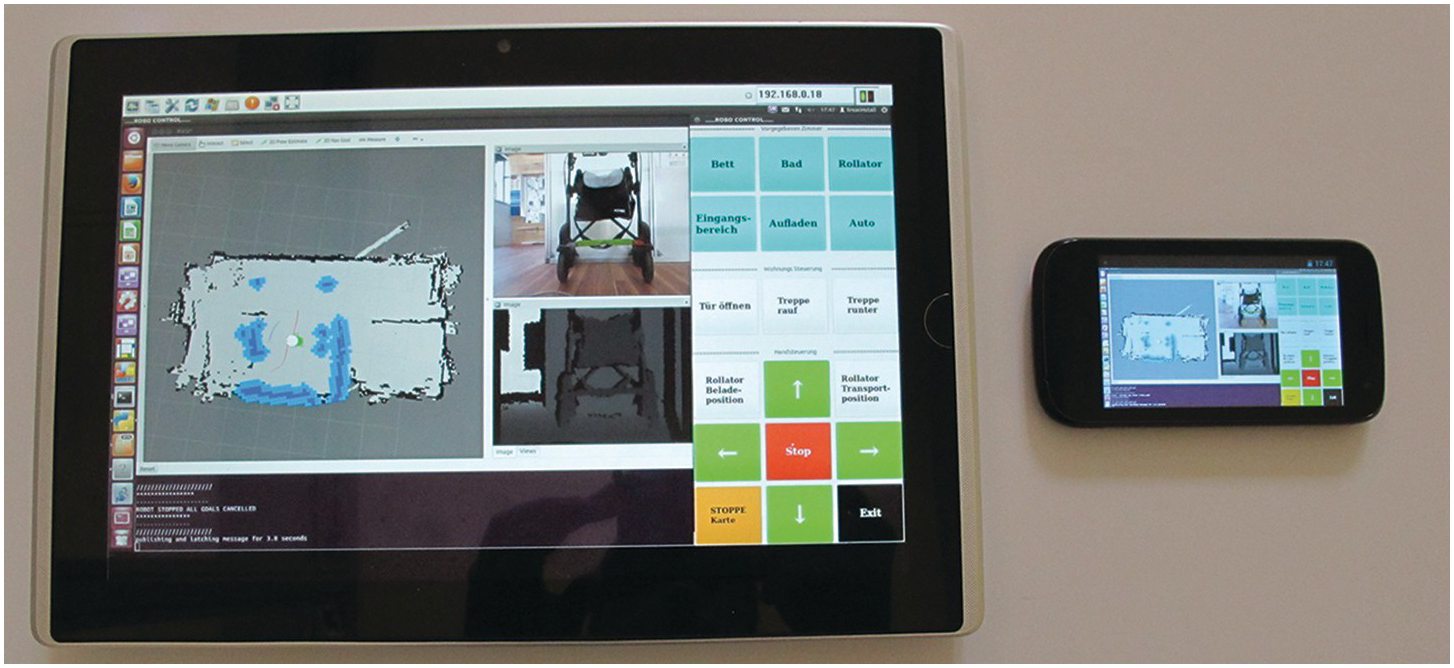
Figure 5.11 Left: A tablet PC with Windows 7 as the operating system. Right: A smartphone with Android as operating system.
The main challenge here is only to find an appropriate interface to control the necessary service task. According to [162], the use of smartphones or tablet PCs is an intuitive way to offer services to the elderly.
Because they lack haptic feedback, touchscreens are not the best solution. Voice control will become an optimal solution, if the matching algorithm becomes more robust. Autonomous and independent working robots demonstrated the highest user acceptance in the test.
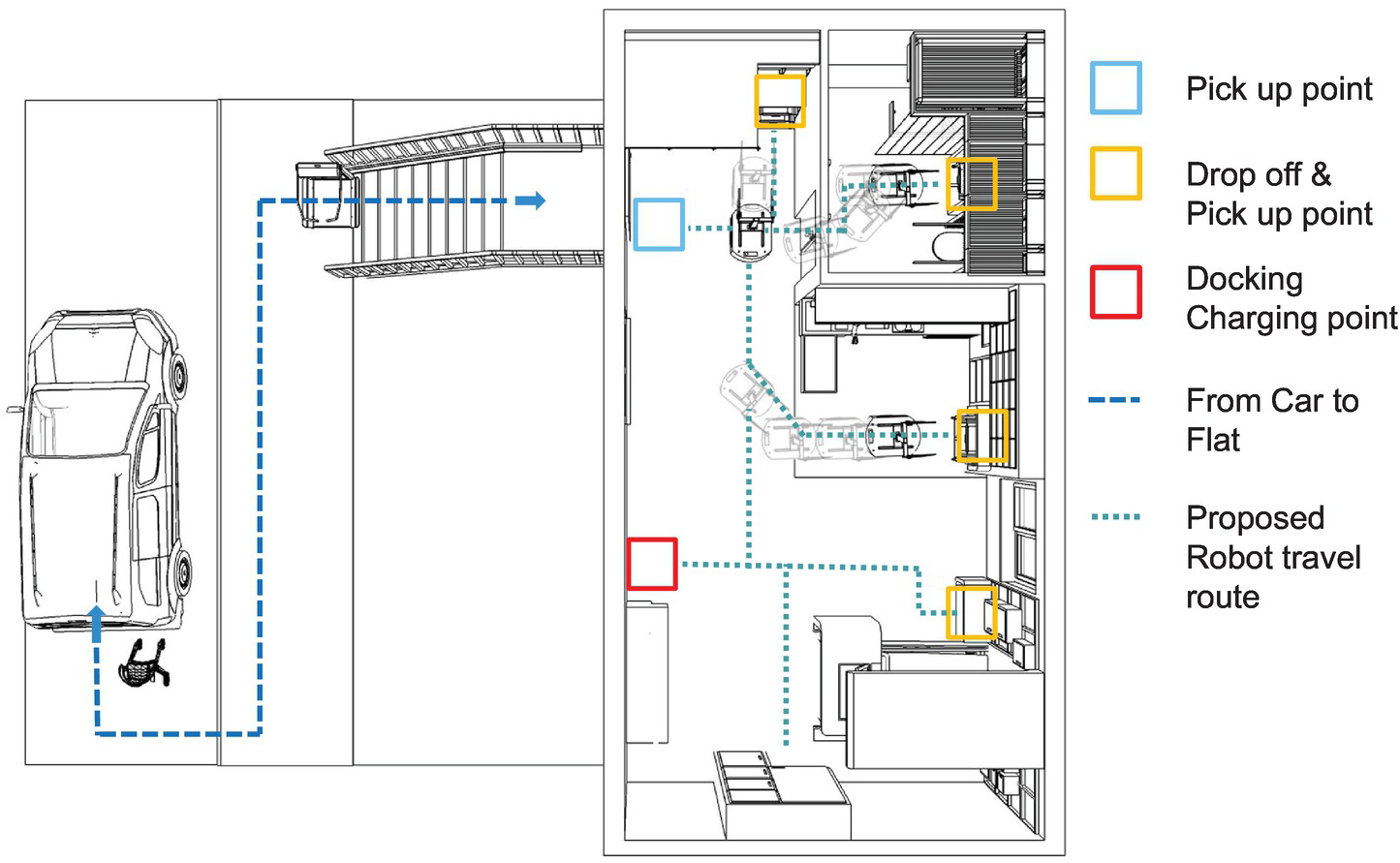
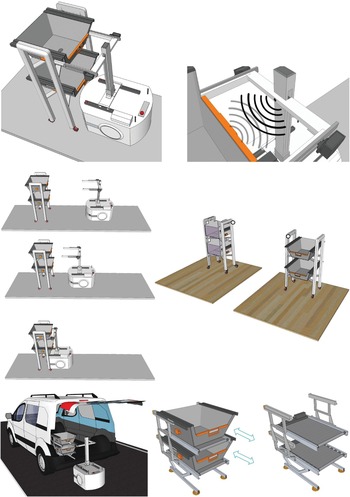
Considering Use Case 2 of Figure 5.9, stairs are a major challenge for the TurtleBot as well as for rollator or wheelchair users. Therefore, transport options have been added to a device, which is named “StairWalker” (see Figure 5.12).

The StairWalker is comparable to a stair lift, with the difference being that there is no existing sitting place. This means that the user has to walk up and down the stairs on his own. The device just supports stair climbing, just like a rollator supports walking. Such devices are important to avoid an accelerated senescence, because if the elderly person continues to climb stairs, muscle will not begin to atrophy according to laws of nature – use it or lose it [163]. However, to enable the user (or the TurtleBot) to leave the apartment with the rollator, an automated transport box has been added, which is 100 percent with the overall indoor system.
This means that the GUI, and also the end user, is able to control the StairWalker and the TurtleBot. Depending on the source code, the TurtleBot is potentially able to call the appropriate shell script commands, depending on his current position on the apartment map. The details on how the interface between the tablet, or smartphone, and the robot has been realized is described by [164].
These prototypical implementations, which have been tested by the elderly in the laboratory test apartment, allowed to simulate several solutions as depicted in Figure 5.13.
Using stronger robots than the TurtleBot would also add the simulated tasks. Depending on the robots’ oriented design, the mobile platform, e.g., the Lynx Adept, could be enabled to carry objects to the car or into the apartment. For this purpose, special add-ons have been designed, as depicted in Figure 5.14.
5.4 Project USA²
Project USA² (Ubiquitäres und Selbstbestimmtes Arbeiten im Alter) aimed to develop decentralized work stations, which allow the retired elderly (or fragile) to take active part in the work life. The project focused on retired engineers for a period of one year with support of up to € 300,000 from the BMBF. Figure 5.15 demonstrates the basic idea of this project.
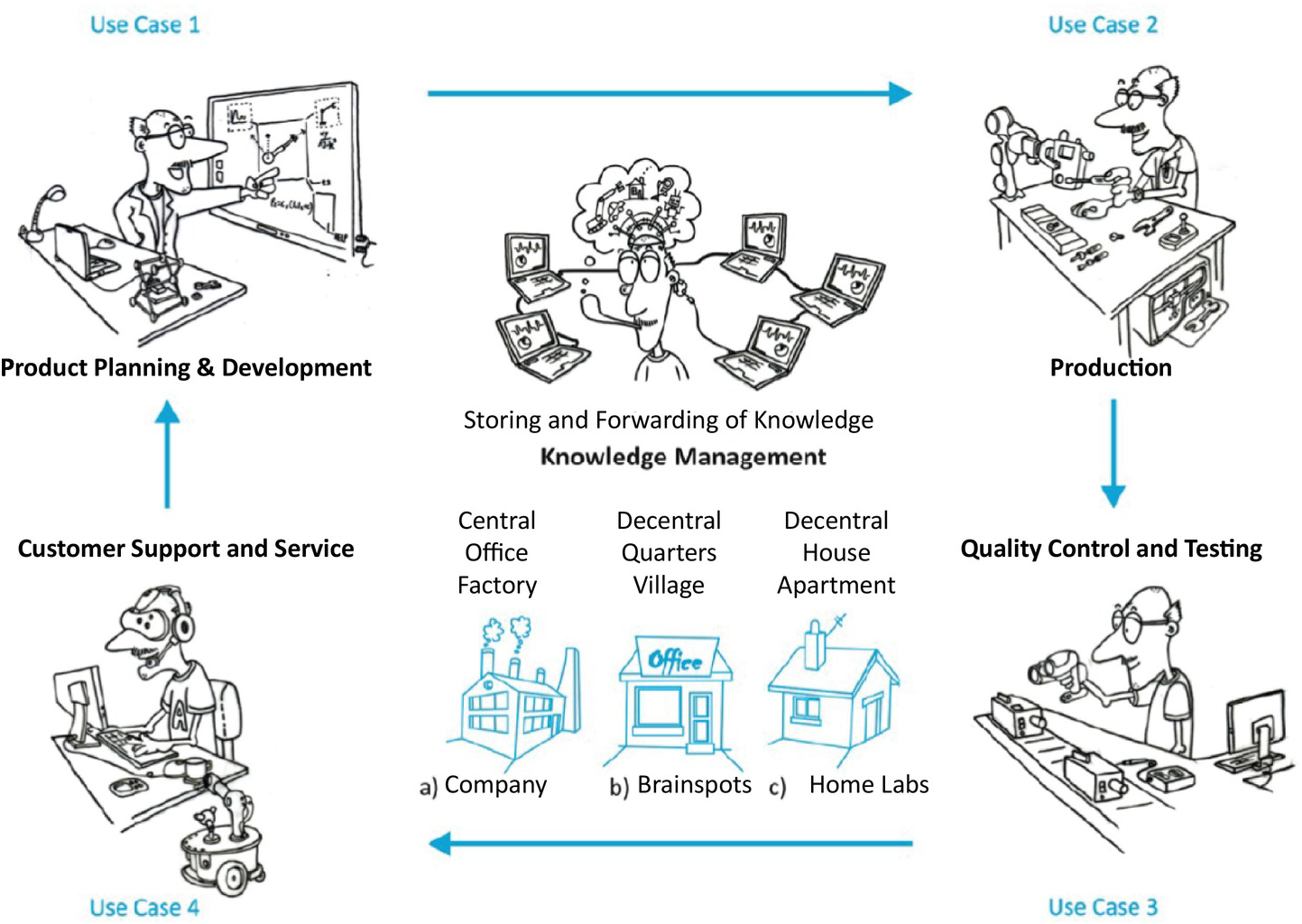
As it can be seen in Figure 5.15, this project considered the whole lifecycle of the product, starting with the product planning, development, quality security and testing up to service support. By recording and sharing the knowledge, robotic elements should learn basic movements or tasks, in order to support the elderly. The prototype concept was developed for three different scenarios: (a) for use as a modern production station in companies, (b) for home use, and (c) for use in “Brainspots.” A Brainspot can be seen as a decentralized manufacturing corner, where the companies and communities provide the elderly in a neighborhood access to this workstation to allow them to stay active in their former employment.
At the same time in countries like Germany, it is expected that by 2030, approximately 7 million fewer employees will exist as compared to today. This means that within the next years, the gross national product will reduce by 16 percent [165], including a large knowledge loss, because of the retirement of highly experienced employees. There are existing studies (e.g., [166]), which prove the abilities of the “young.” By keeping the elderly person especially mentally active, the process of senility should be slowed down [167], [168]. This means that this approach leads to a “win-win-situation”, as the economy together with the elderly and their health benefit.
In order to allow for a proof of concept laboratory test, new technologies like 3D scanning and 3D printing, have been used for the production. Also, in this “mini home-factory,” robots support the work. A robotic arm (Jaco-arm robot [169]) and a logistic platform (for this basic investigation the TurtleBot has been used) have been implemented in the work station.
The overall shape of the workstation orientates on the ergonomic structure of an airplane cockpit. The pilot in an airplane cockpit can easily reach each important switch. This leads to the specific design of the decentralized mini home-factory, as shown in Figure 5.16.
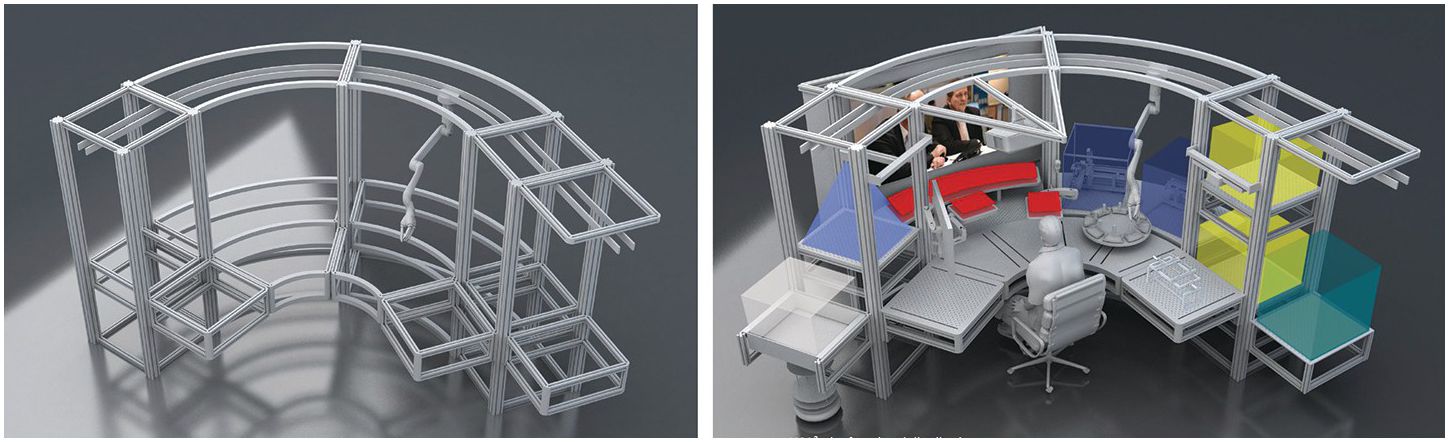
The basic frame has been designed using Maytec profiles. The surrounding shape, including the user head structure, allow the future inclusion of modules for different tasks. Furthermore, the workplace can be segmented in four different areas, where for each area, a different main task was conceived (as presented in Figure 5.17).
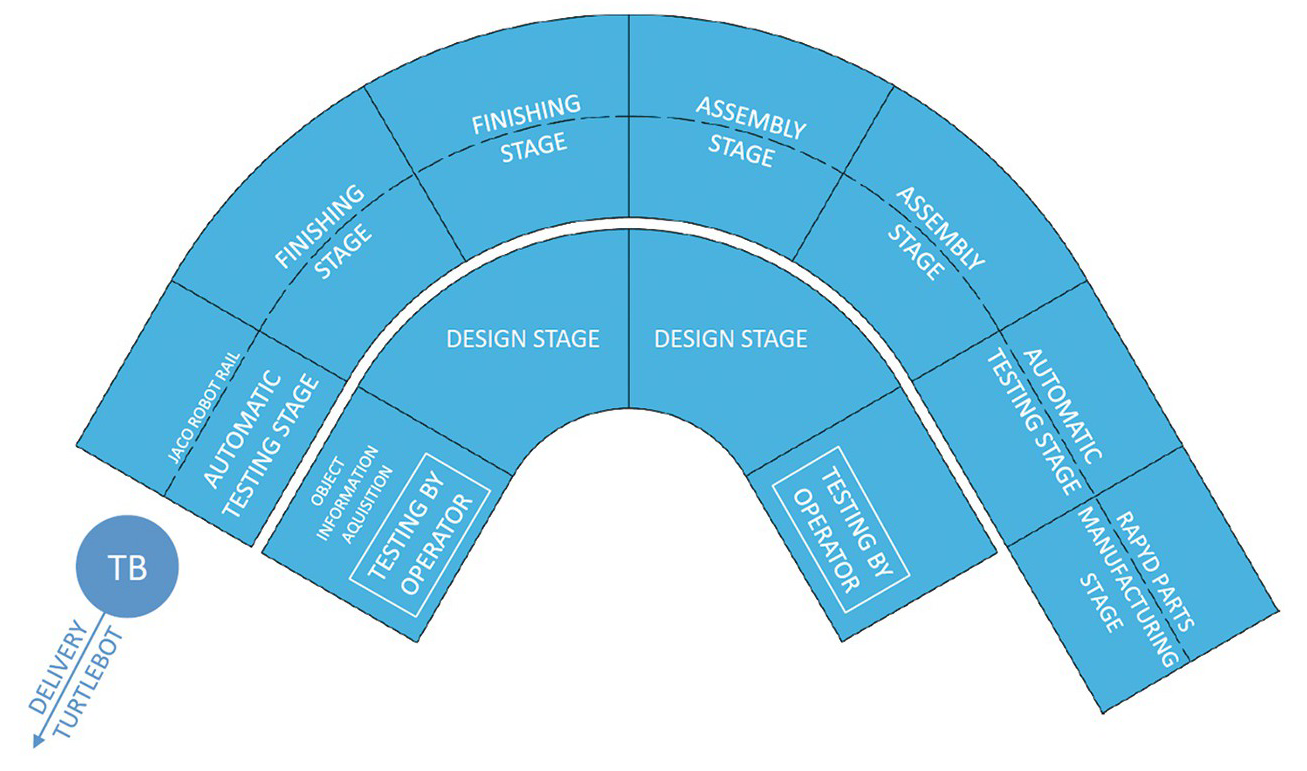
Figure 5.17 The different segments of the “mini home-factory,” with their task objectives.
The front table also serves as a security obstacle, as it blocks the user from easily reaching the back area of the workstation where the automated testing, finishing, assembly, etc., takes place. The reason therefore is the idea that in this area where automated processes take place, the user can easily be harmed (e.g., by accidents or by misuse).
The prototype depicted in Figure 5.18 has been built in order to investigate the possible integration of different modules which will lead to the mini home-factory.

The workplace aimed to enable elderly engineers (from different fields) to stay active (or become active again) in society. Figure 5.19 shows how the workplace will be implemented, and represents the whole production cycle of a customized handgrip of a walking aid.
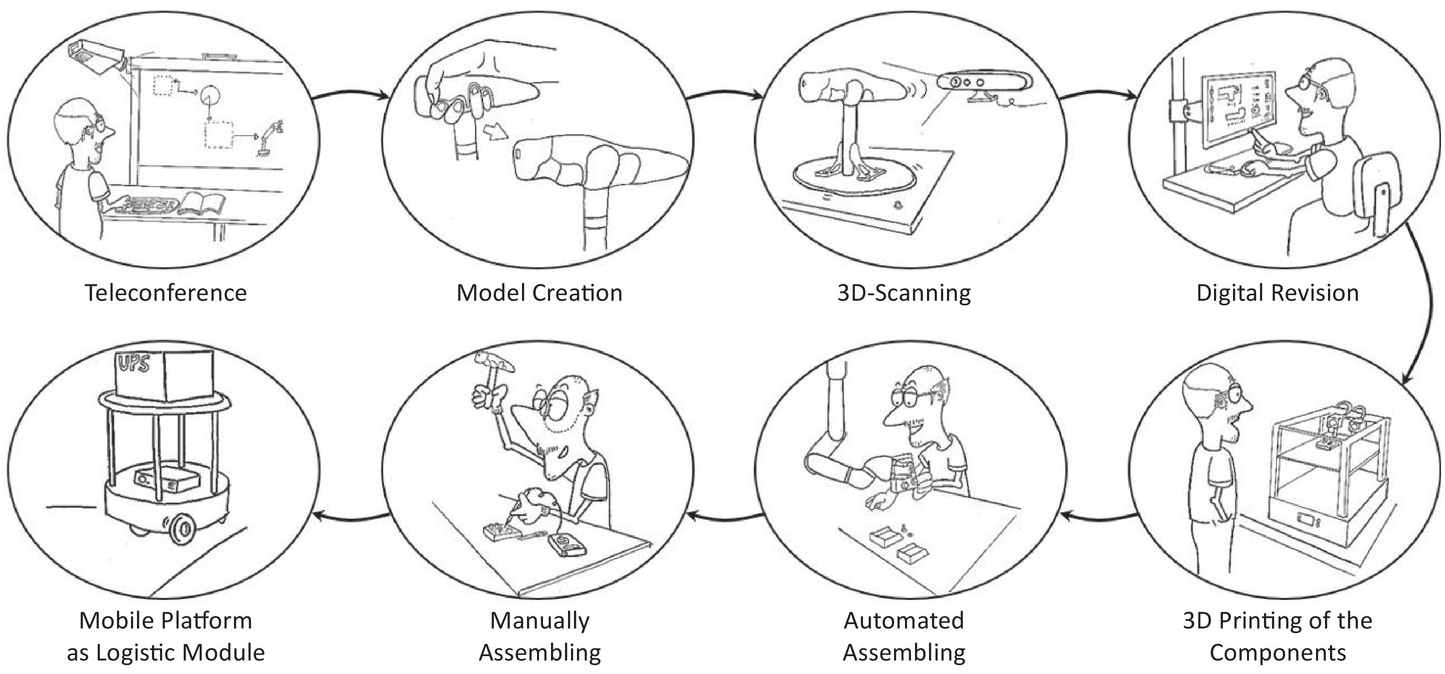
Figure 5.19 The production of an item using the mini home-factory; the process starts with the teleconference module (to receive instructions), followed by building an initial model that will be scanned using 3D scanning technology, and finally digital improvement and adjustment of the scanned result.
The user may attend work tasks, production discussions as well as meetings via the telepresence module consisting of a beamer, a beamer wall, and two HD webcams. The two cameras are necessary because of the possibility to sketch something (e.g., on a sheet of paper) and to immediately show it on a specific table to the audience by using picture-in-picture mode. As soon as the user knows the work task, the preparation of a model using CAD software is necessary. In order to allow an easy and fast modeling process, e.g., by using a small scaled sample, the user could scan the object and immediately receive the basic contour data.
For the manufacturing, a 3D printer (German RepRap X400) has been used. A robotic arm on the rail could drive to the printer and grasp in it, in order to transport the object to the user (as depicted in Figure 5.20). To manage the transport of materials or the final product, a logistic platform was used.

Figure 5.20 Left: 3D Printer X400 from German RepRap. Right: the 3D Pinter interacting with the robotic arm Jaco.
In order to allow the user to interact with this backstage area without coming too close to it, the robotic arm, Jaco, services as a secure interface. Jaco is mounted (as depicted in Figures 5.16 and 5.18) on a rail at the top of the workstation. From here, the arm can move in each of the back segments of the “mini home-factory.”
Even today where the use of technology and robotics is much easier than 40 years ago, it can be challenging for an elderly person to efficiently use a robotic arm. An intuitive control option had to be found. Three different control options (automated tasks, virtual joystick, and gesture control) for the robotic arm have been implemented and their user acceptance further investigated in a laboratory test. The overall control, where the user decides the most preferred control, is depicted in Figure 5.21.
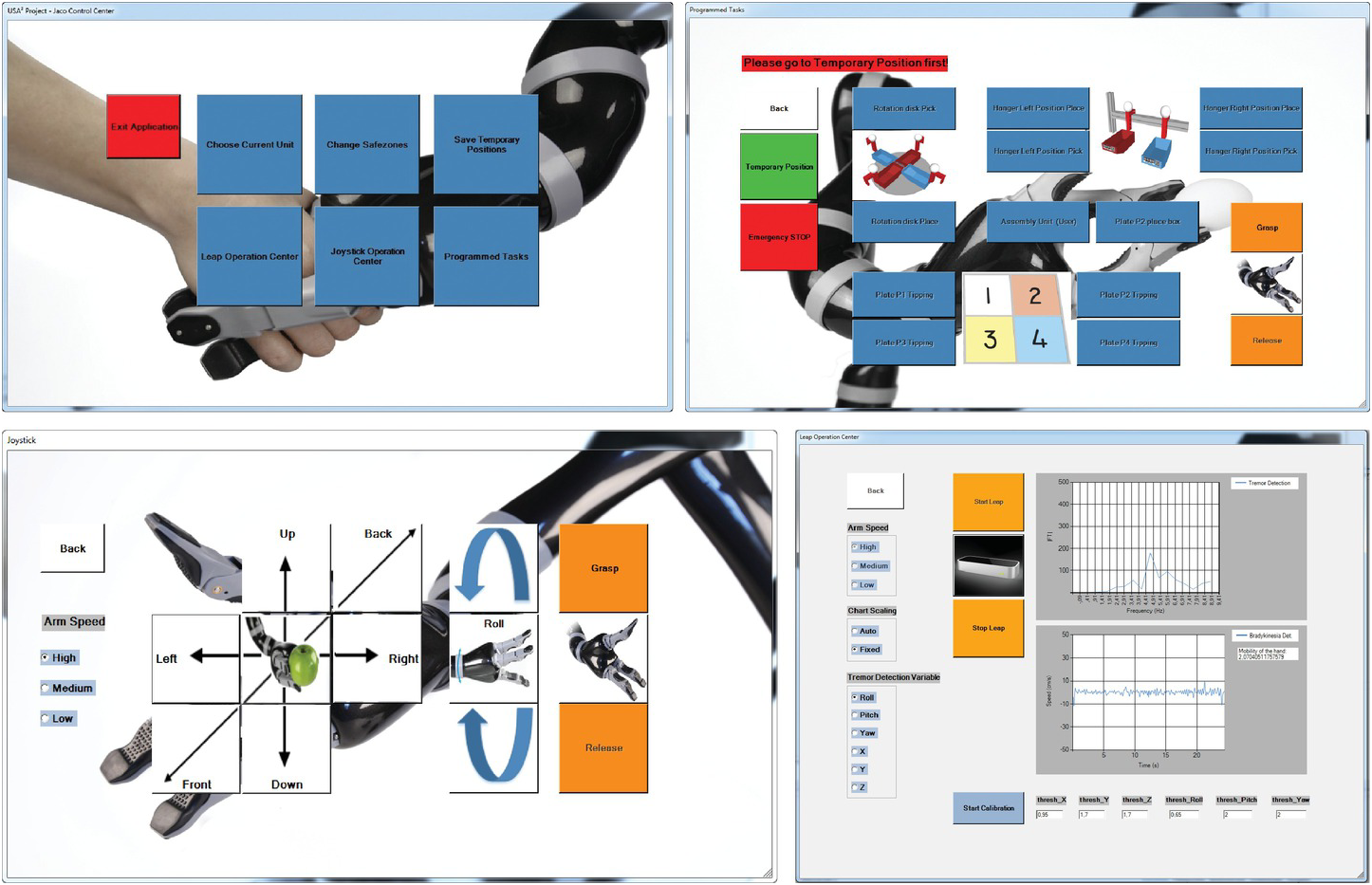
Figure 5.21 Graphical User Interface (GUI) of the Robotic arm. Top left: Start GUI, where the user selects the control mechanism, Top right: GUI allows execution of automated tasks, Bottom left: GUI allows to directly navigate the robot by arrow buttons, Bottom right: GUI allows arm control by gesture, the GUI displays the physiological measurements which are executed in parallel.
The control option to use automated task and the joystick control represents already known control options. The gesture control represents a new innovative way to control the robotic arm (visible in Figure 5.22). The Leap motion sensor has been used as an interface to recognize the user hand and send the movement information to the robotic arm [169]. This allows an intuitive use of the robot, which elderly of all education classes can use.

Nevertheless, the complexity of the possibilities of this workplace was still so large (comparable with the complexity of a car) that the user requires guidelines. Therefore, the Augmented Reality Device, Vuzix, has been used (visible in Figure 5.23). By contour recognition, as well as 2D barcodes, the Vuzix M100 could instruct the user on how to use the different applications (e.g., by tutorials with the loudspeaker and the display), giving hints as to where the switches are, etc. [170].
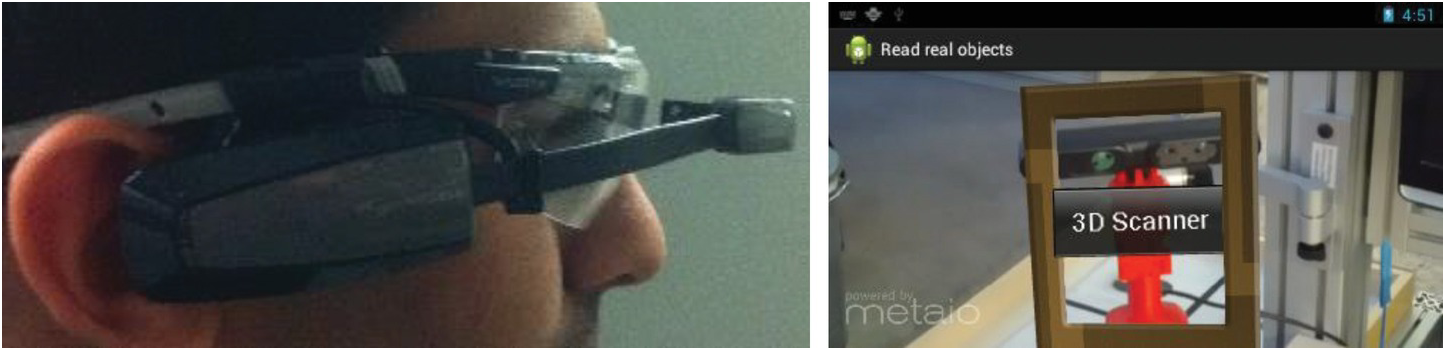
This system offered a unique opportunity to implement a physiological measurement. While the user is working with the robots using gestures (this keeps the elderly active and healthy) and gets guidelines by the AR device Vuzix M100, the tremor of the head and the hand can be analyzed [170], [171]. This is possible as the Vuzix M100 has gyroscopes and accelerometers implemented. For hand analysis, a numerical differentiation is necessary to receive the user hand movement acceleration from the position values of the hand. The measurement possibility has been demonstrated by display of the appropriated GUI as shown in Figure 5.24.
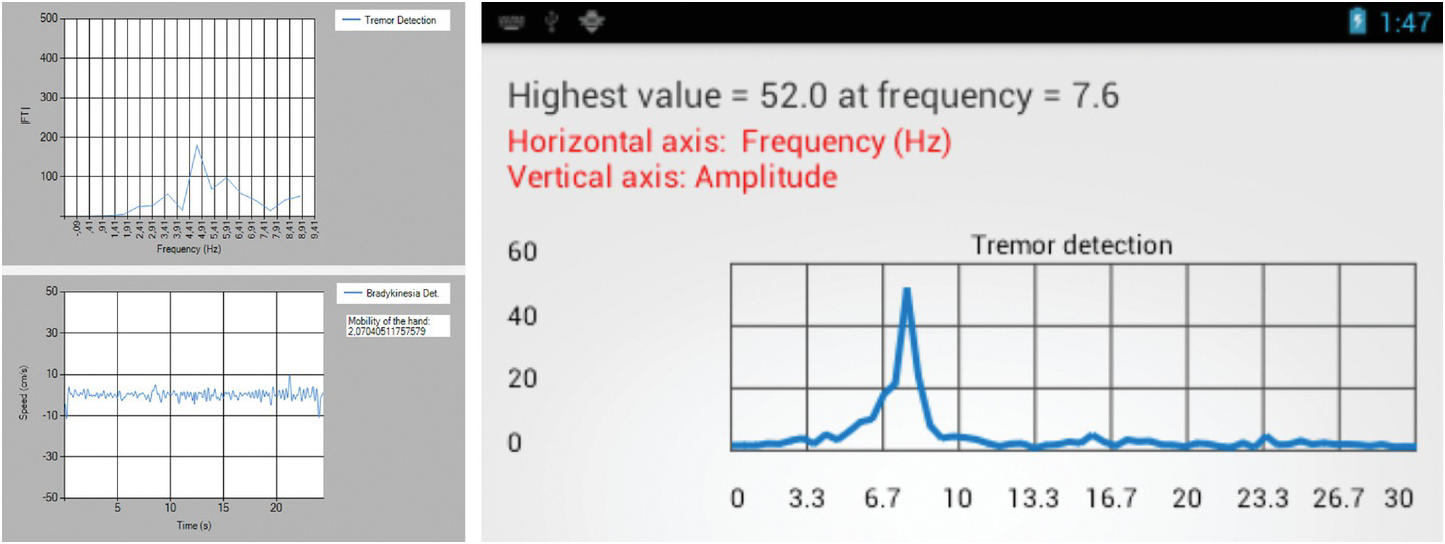
On a second stage, in order to estimate a possible bradykinesia, not only the tremor, but also the speed of movement was analyzed according to A. Salarian et al. [172].
The information about tremor and bradykinesia of elderly is of interest because they are indicators of nerve diseases like Parkinson’s disease [173]. These diseases mainly affect elderly above 55 years (i.e., the target user group) and the prevalence has increased over the last years.
Furthermore, Parkinson’s is not the only disease that can cause symptoms like tremors. Several diseases may also lead to these symptoms, but they differ in their frequencies and amplitudes, e.g., essential tremors [173]. By recording the analysis of the user movements and combining with telemedical applications, an early intervention can be realized in the future. This would increase the life quality mainly because currently there is no known recovery method for diseases such as Parkinson’s, as it is only possible to slow down their progress. Therefore, the earliest the intervention process starts, the more that life quality in old age can be secured.
5.5 Project LISA-Habitec
The project LISA-habitec (Living independently in Südtirol Alto-Adige through an Integration of Habitat, Assistance, Bits and Technology by a value System based on local Resources) is a follow-up project based on LISA (see Section 5.2). In this project, not only one apartment area is considered (as in LISA), but rather a smart LISA AAL wall for all apartment areas is developed. The predefined apartment areas from LISA have been incorporated into this project, including the knowledge about the necessary space which enabled understanding of the basic concepts at the start of the project (Figure 5.25).
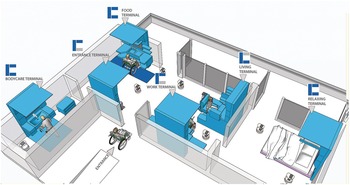
Figure 5.25 Basic concept of the LISA-habitec smart AAL walls.
Here, the most challenging aspect for each apartment is to define the area specific service function which allows the elderly to even stay alone at home. For this purpose, a basic analysis was done at the very beginning of the project. The elderly both at home and in care homes were asked about their preferred support and needs.
Table 5.1 gives an overview about the potential functions and service modules considered from the beginning. Additionally, user benefit has been evaluated by interviewing the elderly.
Table 5.1 Service Functions of the Different Smart AAL LISA Walls – Bathroom and Kitchen
| Service Functions | User Benefit | |
|---|---|---|
| Basic Wall | Emergency call | 5 |
| Fall detection | 5 | |
| Medication dispenser | 3 | |
| Vital data measurement | 3 | |
| Communication | 4 | |
| User interface | 4 | |
| Central controlling unit/house technic | 3 | |
| Data platform for access of several user | 4 | |
| Multifunctional robot | 3 | |
| Bath room | Sink | 3 |
| Mirror | 3 | |
| Storage options/bathroom cabinet | 3 | |
| Towel rail | 3 | |
| Handles and rods to hold on | 4 | |
| Height adjustability | 4 | |
| Light and lightning atmosphere | 3 | |
| Module for cleaning denture, teeth brush, etc. | 3 | |
| Assistance with reaching objects | 3 | |
| Heat radiation | 4 | |
| Seating accommodation | 4 | |
| Module for measuring weight/body fat, BMI, temperature | 3 | |
| Overflow sensor | 4 | |
| Automated regulation of the sink water temperature | 4 | |
| Automated regulation of the water temperature | 4 | |
| Support with applying cream | 4 | |
| Full body dryer | 4 | |
| Kitchen | Automated shut down of devices | 5 |
| Automated detection of security relevant environmental parameters | 5 | |
| Seating accommodation | 4 | |
| Height adjustability | 4 | |
| Repair and maintenance services | 3 | |
| Integration of eating opportunity | 3 | |
| Assistance in serving food | 3 | |
| Light and lightning atmosphere | 3 | |
| Dispenser/magazine for liquids | 3 | |
| Cooking machine | 3 | |
| Module for the automated cutting of food | 3 | |
| Automated reordering of food/catering services | 2 | |
| Assistance with reaching objects | 3 |
Once all potential service functions were collected, they were additionally analyzed according to innovation, technical feasibility, expected material, and production costs, expected benefits to all stakeholders etc. This approach allowed for ranking of the collected ideas regarding the service modules. The objective in the project was to come up with three new and highly innovative functions for each apartment area. The smart LISA AAL walls would offer new functions without staying in competition with already existing products.
Within this project, several prototypes as shown in Figure 5.26 have been developed.

The kitchen and bathroom areas showed that it is more useful to develop a table and bed containing the different modular service functions instead of developing a smart AAL LISA wall.
Additionally, to this overall shape development, several service modules were also developed. These included new service module prototypes that give the smart environment an advantage over its competitors. These newly invented prototypical service modules are describedin the next section.
5.5.1 Coat Dressing Aid
In old age, wearing the correct cloth is quite important. For example, wearing a very thin coat in winter can trigger influenza, which is faster and easily distributed nowadays. For the elderly, this is very risky [174]. Often, some have to briefly leave the apartment (e.g., to throw away garbage). If it is too exhausting, painful, or difficult to slip into a coat, the elderly will go out without one. The cold makes people rush and in worst cases may lead to accidents. Once the mobility decreases, as expected while aging, wearing a coat becomes challenging. Age-related diseases like Parkinson’s and osteoporosis can lead to the necessity of requiring a second person (helper/care giver) to dress the affected elderly when the need arises. Also, in old age, the elderly will sooner or later be alone, and this aspect can already lead to a dependency that can only be properly treated in a care home. Therefore, the prototype shown in Figure 5.27 has been developed.

With this device, only minor dexterity is needed to put on the coat. A foot switch triggers the device, which then drives to the user in order to attach the coat. As soon as this is done, the senior lays his or her hands in the coat arms and presses the foot switch again. By appropriate driving of the two actuators attached at the top, the coat gets drawn up and moves forward at the end, and the user attaches the coat using the clamps. Therefore, the coat first gets laid on the device as shown in Figure 5.27. This allows the device to clamp the collar using clips. Once this is done, the coat will hang on the device and follow the body contour. The device must be setup individually to the user’s height. At the end of the procedure, the user presses the foot switch in order to move the device to its parking position at the very top. By applying force on the clips, the collar slips out and the user can continue with his business.
5.5.2 Contactless Fever Measuring
Health is of major importance to those who are fragile, and it is therefore advantageous to know about their current health conditions. For example, fever mostly occurs when the immune system is defending the body against pathogens [175]. Recording body temperature over time gives a summary of health condition developments and aids in the prevention of complications, e.g., to avoid developing pneumonia following a minor infection. Although everyone in their life has had their body temperature measured, there is a possibility of making mistakes in the measurement. Furthermore, measuring fever can be time consuming, making it very inconvenient to track body temperature. Meanwhile, there exists several devices which can measure body temperature on the forehead or ear drum via infrared [176], [177], [178]. Nevertheless, who has time and the intention to track the measurements frequently over days and weeks? Additionally, hygiene must be considered, especially when the device is used on several people [179].
Therefore, a module for contactless fever measurement has been developed. As shown in Figure 5.28, this module is hidden inside the smart LISA AAL bath wall.
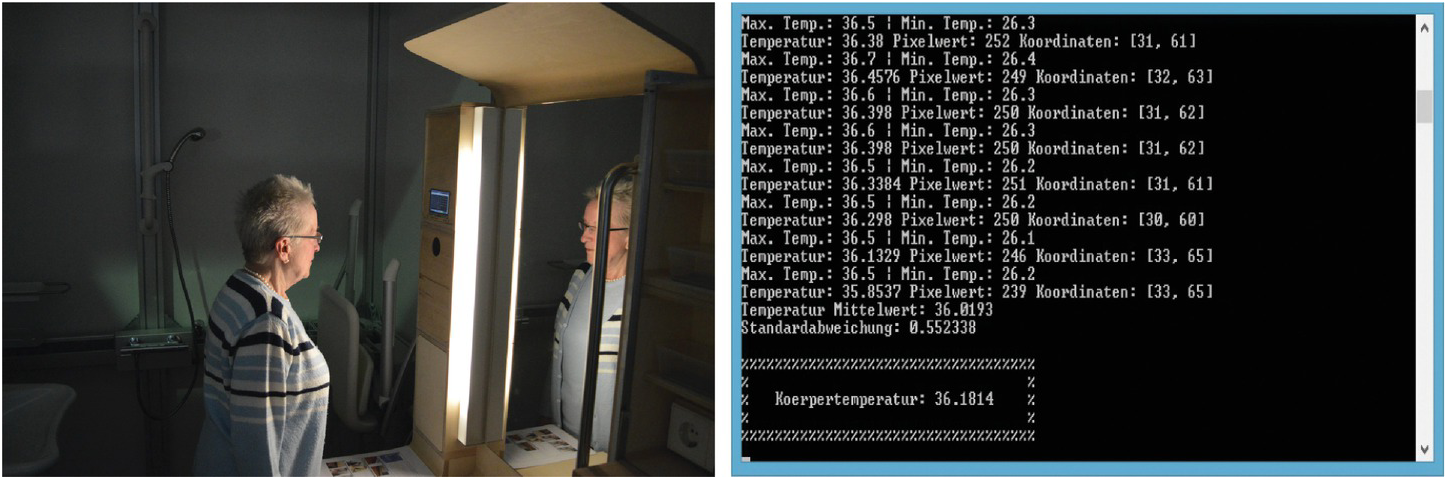
Figure 5.28 Left: The unobtrusive measurement of body temperature. Right: Display of the results for demonstration purposes.
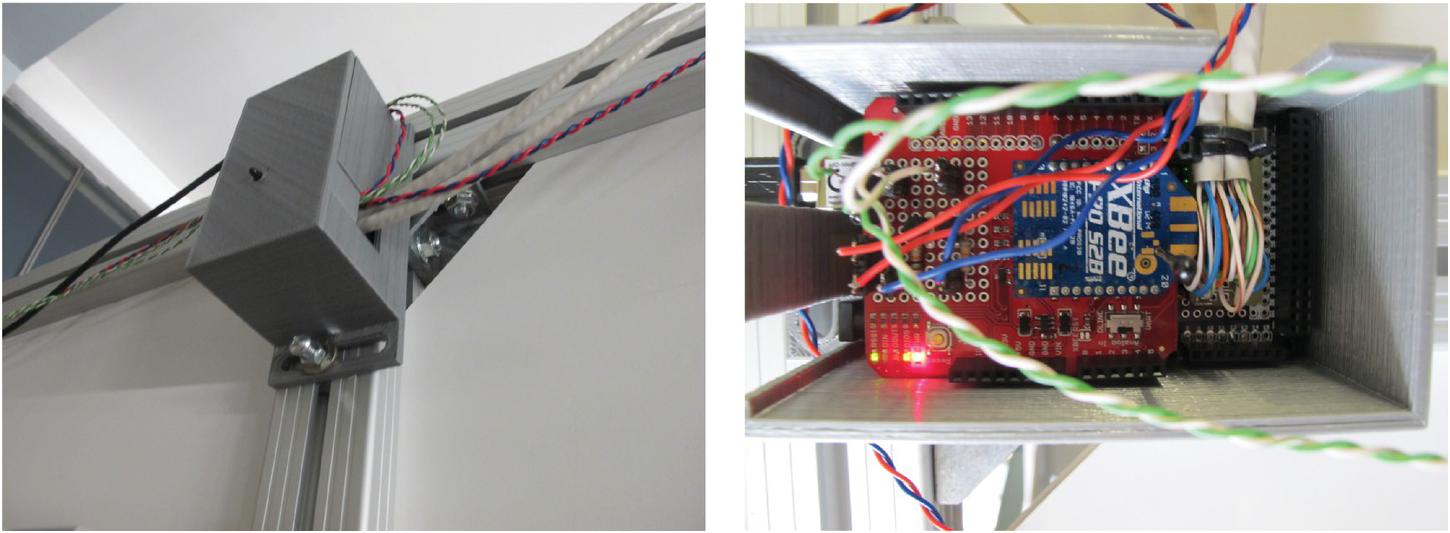
The module permanently tries to measure body temperature; as soon as a human face is detected, the device searches for the forehead and captures the temperature. To do this, a thermal camera is used. For the forehead finding algorithm, a single-board computer (BeagleBone Black) has been connected to the thermal camera to read out the images and carry out analysis (see Figure 5.29).

In order to avoid many wrong measurements, several measurements are detected and analyzed but get cancelled for the final result calculation according to stray bullet (see Figure 5.28). The display serves just for demonstration (or prototypical) purposes. In order to enable the module, the modular interface ability, as in Section 5.1, an XBee antenna has been attached.
XBee antennas, when compared to Bluetooth and Wi-Fi, operate on the principles of radio waves, and have a much larger transmission distance. Like Wi-Fi and Bluetooth, this module offers access securities like ID numbers, passwords, and encryption of the transmitted data. Their high transmission distance and small size allows a straight forward, and according to their lower popularity compared to Wi-Fi, more secure wireless data transmission.
Details regarding the development and the functionality of the contactless fever measurement for this specific purpose can be read in [180].
5.5.3 Contactless ECG Measuring
The possibility to measure unobtrusively and without any direct contact has many advantages. However, this is not possible in most cases. For example, in ECG measurements, which belongs to one of the most common and important measurements in medicine, there does not exists a way to measure without contact. Normally, at least three to four electrodes (for one to six leads, see Chapter 2) which must be placed at appropriate spots in order to enable a comparable measurement are necessary.
Skin irritations are often the result of the self-holding glue electrodes. Therefore, capacitive electrodes are of high interest for the project. They have the potential to measure the ECG even through clothes. To verify this, a prototype using the BeagleBone Black for the user interface, Arduino with appropriate ECG shield (ECG shield from Olimex), and capacitive electrodes has been used to investigate the use of this technology in the home environment (see Figure 5.30).
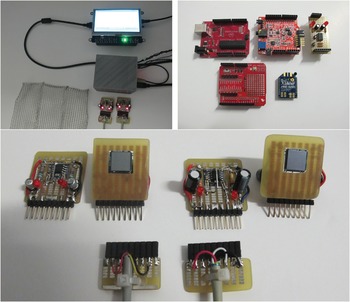
Figure 5.30 Top left: The capacitive ECG prototype. Top right: Wattuino, ECG shield and XBee shield, as well as drive ground plane circuit. Bottom: Capacitive electrodes as equalized interface to the prototype.
As soon as the prototype was set up, it was implemented in a wooden armchair as shown in Figure 5.31.
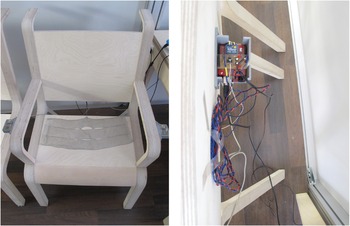
Figure 5.31 Left: front side of the implemented capacitive ECG. Right: the unobtrusive attachment on the back of the chair.
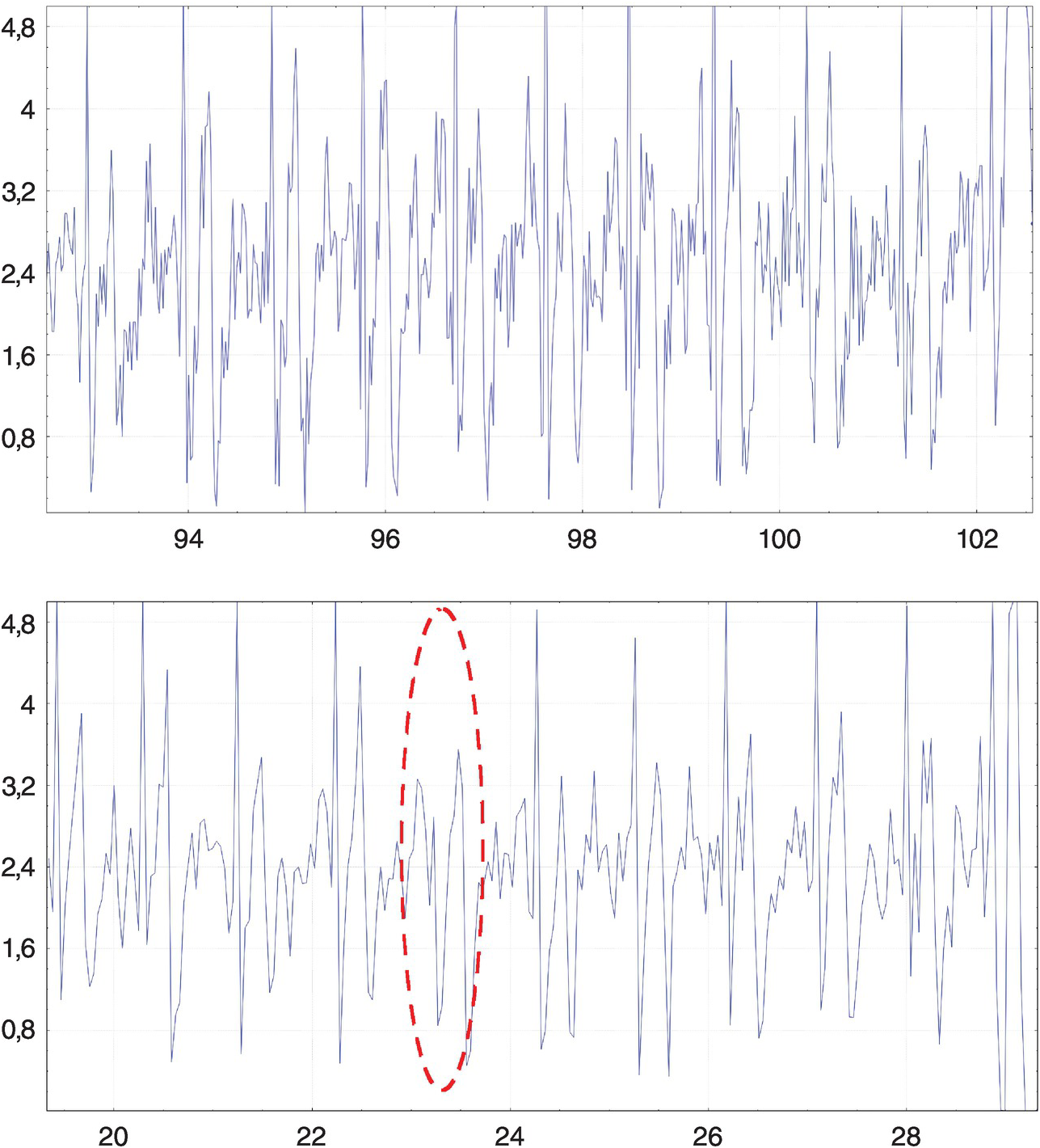
For this system, two electrode chips (PS25203B and PS25201B) were purchased and compared. The instigation of their potential regarding ECG signal quality (depicted in Figure 5.32) shows that at direct skin contact, the signal quality is even much better than using normal electrodes. Additionally, measuring through clothes is possible. Nevertheless, the electrodes are very sensitive and capture early noise (e.g., from the power sockets in the room). To avoid this issue, it is necessary to shield the system properly [181].
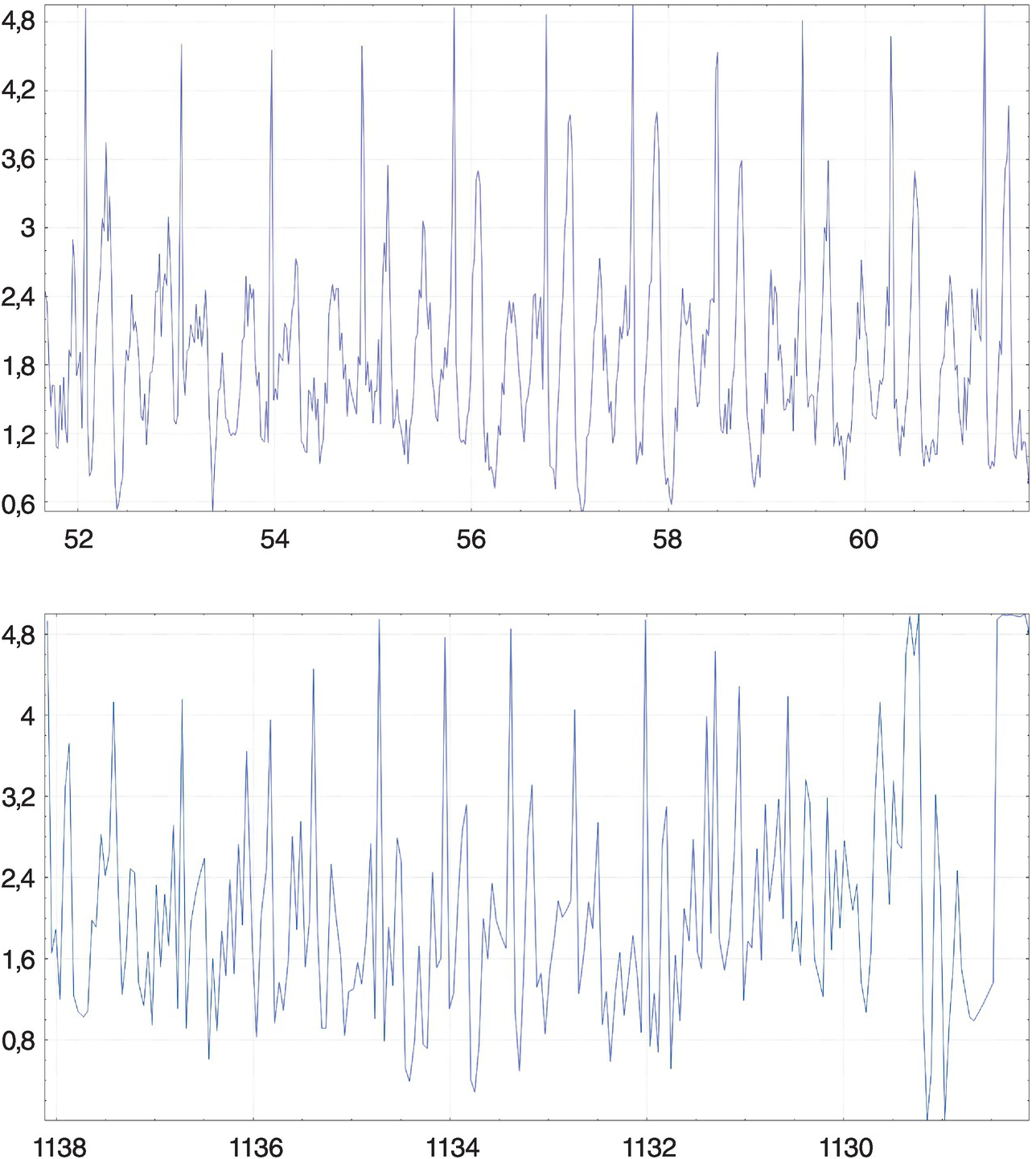
Figure 5.32 Top: ECG measurement with direct skin contact. Bottom: Measurement through a pullover on the chest.
Here also, the XBee antennas were used in order to investigate the potential possibility for real-time data transmission. To do so, the ECG measurement was recorded and compared with different modular settings.
While the results showed that the XBee modules are able to measure, the data transmission is too slow and down samples the sample frequency. This sample frequency down sampling leads to a reduction in the signal resolution. The outcome is, as shown in Figure 5.33, that not all heart peaks can be reliably be detected. Therefore, instead of transmitting the whole ECG signal in real time, the XBee will focus on transmitting just the end results (e.g., the pulse). The BeagleBone Black is fortunately able to store the ECG signal, in order to allow a detail investigation if necessary. For this purpose, the stored data must be read out using, e.g., USB sticks.
5.5.4 Fall Detection
Falling is a major problem, even for the young and healthy. However, falling risk increases in old age due to balance issues. Several systems to detect a fall exist (e.g., accelerometers and gyroscopes). Such systems can be implemented in mobile phones and smartphones as well as in augmented reality devices (e.g., VUZIX M100). Also, sensor mates and “SensFloor” exist [182]. However, SensFloor is the only system which is not a wearable but can reliably detect a fall. Wearables and mates always have the risk that a person is either not wearing the device or is falling next to it.
The SensFloor is based on capacity, similar to smartphones. Unlike pressure sensors, the capacitive sensor is covered by the ground, which protects the sensible sensors. However, there is one big disadvantage: the SensFloor is not usable in the bath. Here, special water mates are necessary, but both approaches are costly, and therefore, a cost-efficient alternative has been investigated. The idea here was to use line lasers that can shoot on up to 15 photo resistors. These settings have been tested in a laboratory test apartment as depicted in Figure 5.34.
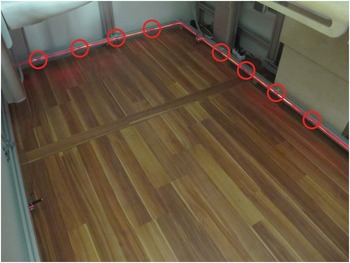
Figure 5.34 Photo resistors of the falling detection service module.
The photo resistors are attached to an ArduinoMega, which is directly connected to an XBee module that forward the information about a fall/not a fall to a server. For the prototype, red lasers were used in order to demonstrate the function (see Figure 5.34). However, in a real home environment, infrared lasers will be used.
In order to reduce the power consumption of the lasers, a transistor driven by the ArduinoMega control allows to switch the laser on, only for the measurement of how many resistors are blocked. If a specific amount is blocked, the system recognizes it as a fall, as it knows that only the blocking size of a human laying on the ground can be able to block these number of sensors. As shown in Figure 5.35, the overall system can easily be installed as a hidden entity.
5.5.5 Shoe Dressing Aid
Although the entrance area is already well covered with potential service modules (see Section 5.2), a special investigation has been done in the entrance area. The objective was to improve the shoe horn. For this purpose, a new kind of shoe shelf has been used. Under the seat of the elderly, a slide was developed which can drive up and enable the user to either put on or remove their shoes (see Figure 5.36).
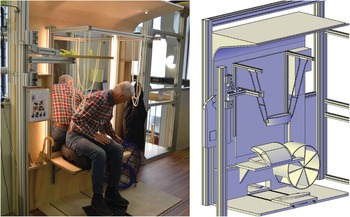
The rotatory shoe shelf reduces the necessary space and allows an ergonomically easy way of reaching different types of shoes. Additionally, the seat offers support when standing up by use of a switch to the right of the user.
In the project, the potential use of an automated rotatory shelf and slide in combination with a belt lift system is investigated. This will not only allow to securely lift an elderly person but also to fully allow an automated shoe preparation step. As a result, this will support the elderly not only in the attract process but also in the shoe exhaust process as done in LISA (see Section 5.2).
5.5.6 Robotic Implementation
In the bedroom module, a drivable table which is thought to serve the user with space for books and tablets or laptops has been implemented. An included power supply socket allows laptops as well as table lamps to work directly in the bed. By automation, the user can drive the table in the appropriate position whenever he wants. As this table is fixed to the bed, only one-directional movements are possible. To automate this kind of furniture is, therefore, compared to a kitchen table, easy. In Figure 5.37, a servant table is shown, which is thought to act as a mobile platform.

Figure 5.37 An automatic moving kitchen table (left) controlled by the robot shown on the right.
Since this set up means that both a two-dimensional movement and a larger payload is necessary, a strong mobile logistic robot is therefore needed. For this purpose, the PIONEER LX from adept mobile robots has been used. The robot is able to carry 60 kg of payload, use a laser as well as four ultrasound sensors (onetime in front and onetime in the back) to avoid obstacles. To prevent the robot from crashing, a bumper in the front immediately stops the current movement. Unfortunately, the introducing interviews (regarding the potential service functions, summarized in Table 5.1) led to the finding that the elderly do not like robots, which obviously seem to be a complex technology (Table 5.2).
Table 5.2 Service Functions of the Different Smart AAL LISA Walls – Bed Room and Entrance Area
It can be assumed that in the next 20–50 years, the attitudes about robots may change. Currently, one solution to this issue is to integrate the robot into a table. As a result, the concerns over robots in the home decreased (the result of a laboratory test), and the mobile table could function in the home in the same way. However, when integrating furniture, it is necessary that needed security sensors (i.e. bumper, ultrasound, and laser) are not covered.
To enable intuitive control of the robot by the elderly, a very simple GUI with large buttons has been realized and finally implemented in the BealgeBone Black (see Figure 5.38).
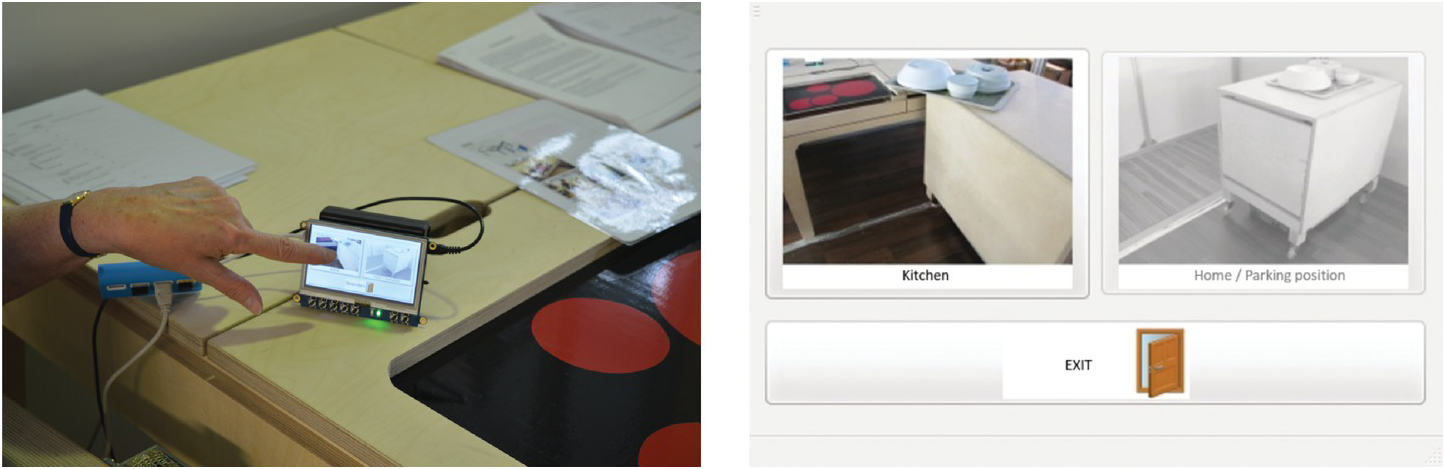
The weak point of this GUI in a real implementation is that the user needs more options in order to navigate the robot; this will in turn reduce the button size (until a larger screen is attached).
5.6 Project REACH
REACH (Responsive Engagement of the Elderly Promoting Activity and Customized Healthcare) is a project for personalized prevention and intervention systems that aim increasing quality of live in old age. For this purpose, sensor networks will be implemented in a user-friendly manner in the environment of the end user to analyze their habits and health condition. The combination of unobtrusive implemented sensors in the environment, wearables, and the actively measured results (blood pressure meter, etc.), allow a seamless flow of information which will later be analyzed by an algorithm to first identify “silent” symptoms to prevent a progress of the disease-causing symptoms.
The prevention program begins by informing the participant of their current condition. Depending on what has been identified, more movements or support in visiting the correct physician and getting the correct treatment is planned. Additionally, the project also considers people who already have an illness, for example from a stroke, fracture (e.g., caused by osteoporosis), or heart attack. Here, the system will aim to prevent a secondary infection or second disease, or as a fall back in the recovering progress.
REACH is split into four subsystems; sensing and monitoring, analyzing and planning, motivation and intervention, and Personalized Interior Intelligent Units (PI²Us).
5.6.1 Subsystem 1: Sensing and Monitoring
This subsystem involves recording, monitoring, and formatting user-specific physical, physiological, and biometric data followed later by a detailed investigation and analysis. Basic sensors which can be used for this purpose for example include accelerometers, gyroscopes (like the implemented sensors in smartphones), bioelectrical sensors (like ECG, EEG, EMG, etc.), electrochemical sensors (like blood glucose meter), optical sensors (like the pulse oximeter), and temperature sensors (ear thermometer to measure on the tympanic) [183]. As illustrated in Figure 5.39, REACH is a solution that proposes its own innovative sensor systems while still remaining compatible with existing sensing systems and technologies (e.g., FitBit).
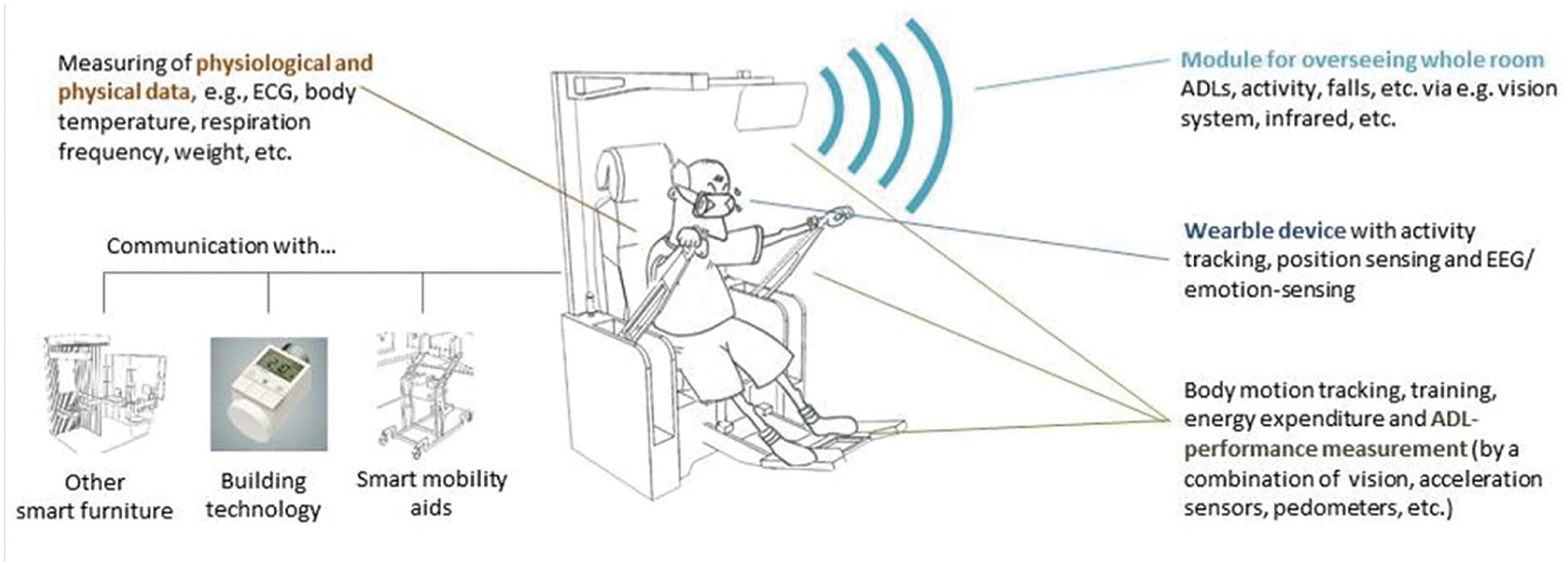
Figure 5.39 Subsystem 1: An example of a stationary furniture implemented with sensor modules that are in communication with wearable sensors so as to capture physiological and physical data of the elderly.
Additionally, Figure 5.39 shows the approach of the sensor system. There are mainly two groups of sensor types: stationary (i.e., fixed and/or embedded) and ambulant (i.e., wearable and/or mobile) sensors. The approach of the modularity, as described in Sections 5.2, 5.4, and 5.5, has to be applied especially for the stationary sensor types.
5.6.2 Subsystem 2: Analysis and Planning
The best measurements are worthless if something is not done. Here, subsystem 2 is used to process and analyze the obtained data from Subsystem 1 in order to generate a holistic user profile with personalized motivation and intervention solutions. The algorithm, which will use the input of Subsystem 1, will generate the user profile while considering the user habits, medical history, and lifestyle. Health-related parameters and recommendation strategies will be enabled to promote healthy habits and improve the overall health condition of the elderly, or at least slow down the design progress.
To do so, this subsystem is split into three parts: First, the data reception module receives the collected and forwarded data from Subsystem 1, and second, the analysis module analyzes the data, which consists of machine-learning, data-mining, activity recognition, recommender systems, and statistical analysis processes and methods (see Figure 5.40).
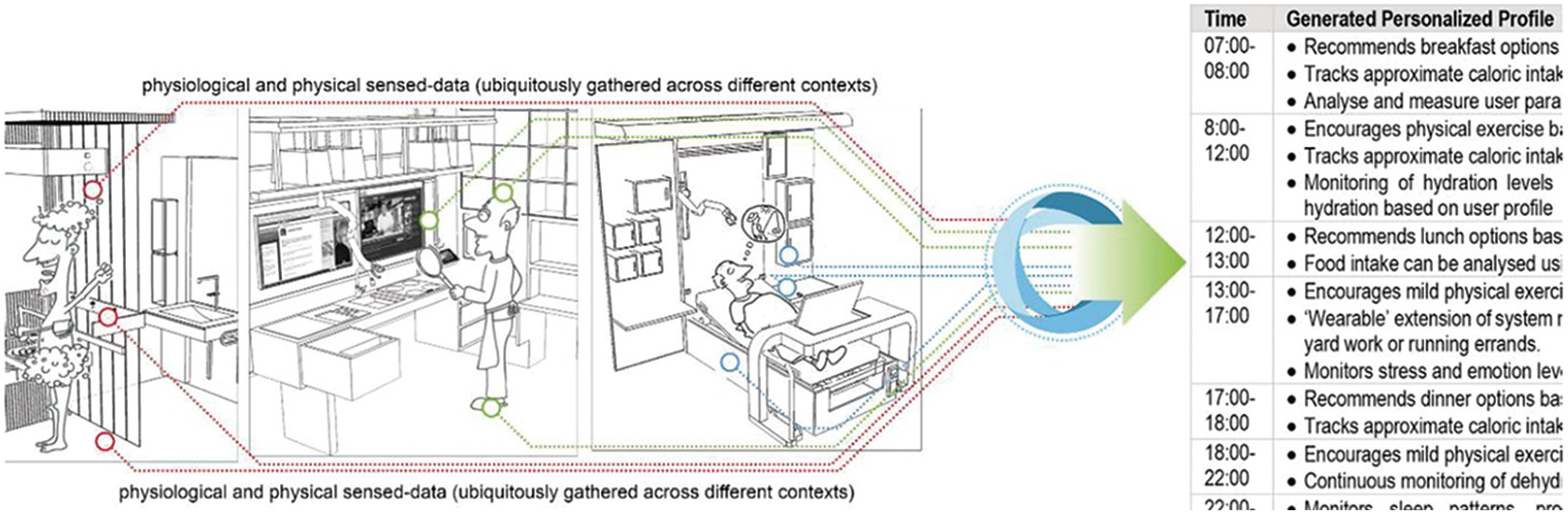
Figure 5.40 Subsystem 2: Physical and physiological data ubiquitously gathered across different contexts and used to generate a personalized regimen.
The third module (the planning module) generates the Inter- and Intra-Personal Profiles generated in the previous modules in order to generate admissible action plans for medical experts, patients, and a variety of autonomous systems. These action plans are then delivered in three different outputs, namely Long-term Correlation, Recommendation Strategies, and Disease Prevention Strategies.
5.6.3 Subsystem 3: Motivation and Intervention
This subsystem consists of intervention solutions (i.e., applications, products, and services) which by considering the conclusions ascertained by the analysis and planning processes of subsystem 2 will adapt to the individual needs of the user. Studies suggest that physical intervention devices not only require effectiveness but also motivational strategies because the user may tend to lose interest/motivation in the device [184] [185]. Therefore, REACH designs physical devices embedded with motivational strategies in their schemes and enables effective motivational considerations for day and night (see Figure 5.41).
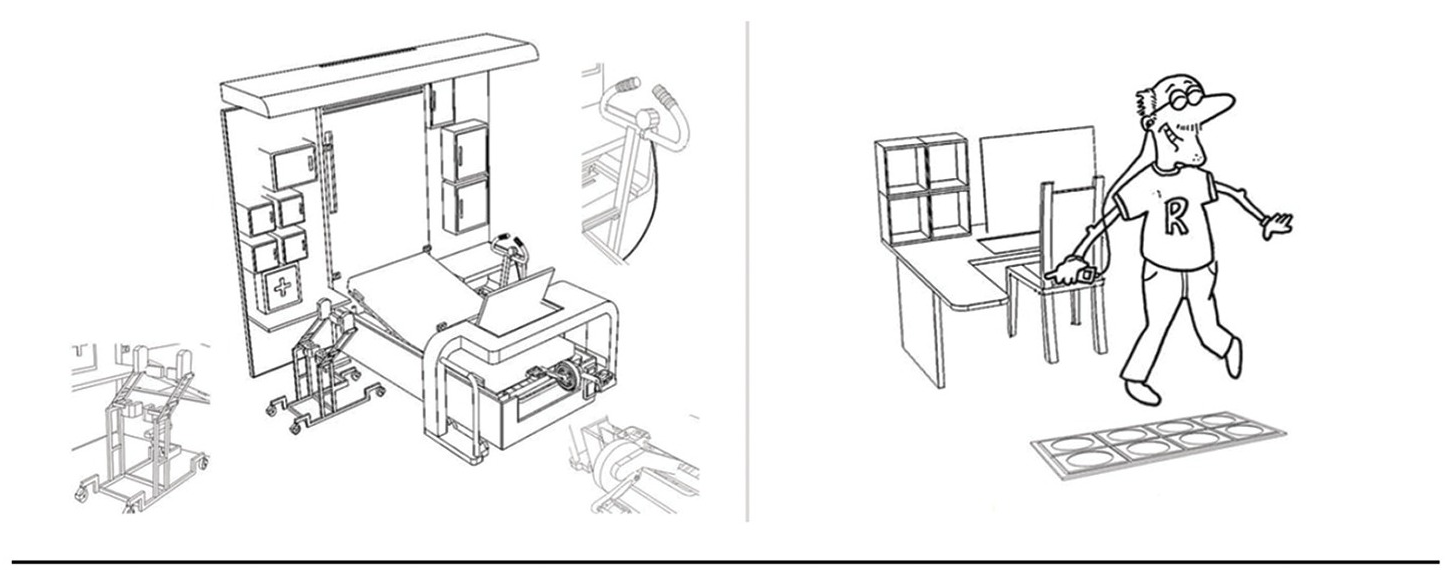
Figure 5.41 Subsystem 3: passive mode interventions for the night (left) and active recommendation intervention for the day-time (right).
These intervention solutions focus on the form of applications, devices, and services, and are divided into four main categories:
Training modules unobtrusively embedded into furniture.
Mobility- and mobilization-assistance devices, both complementary/supplementary to smart furniture and stand alone.
Personalized nutrition via limited 3D printing of certain foods to cater for the palate of the user, while managing healthy nutrition.
Playware to keep the user engaged in a physical and cognitive stimulating way.
In summary, with the guidance of these thematic categories, REACH will provide a variety of products, ranging from furniture-scale to exercise equipment to hand-held playware devices, as well as multifunctional systems for the promotion of activity of all muscle-groups for rehabilitation purposes. Furthermore, the intervention modules have to be designed from beginning on with sophisticated motivation strategies (e.g., suggested by [186]) to keep the user actively stimulated and engaged physically, mentally, and emotionally.
5.6.4 Subsystem 4: Personalized Interior Intelligent Units (PI²Us)
The subsystem of Personalized Interior Intelligent Units (PI²Us) are considered as a type of furniture within the environment (see Figure 5.42). They integrate ambient sensing functions from subsystem 1, and the motivation and intervention modules of subsystem 3 in a manner that enables the use of functionality through one compact element substituting, supplementing, and complementing the existing furniture (e.g., directly implemented into the bed). The PI²Us have to be seamlessly integrated to ensure that technology operates effectively and imperceptibly in the background.
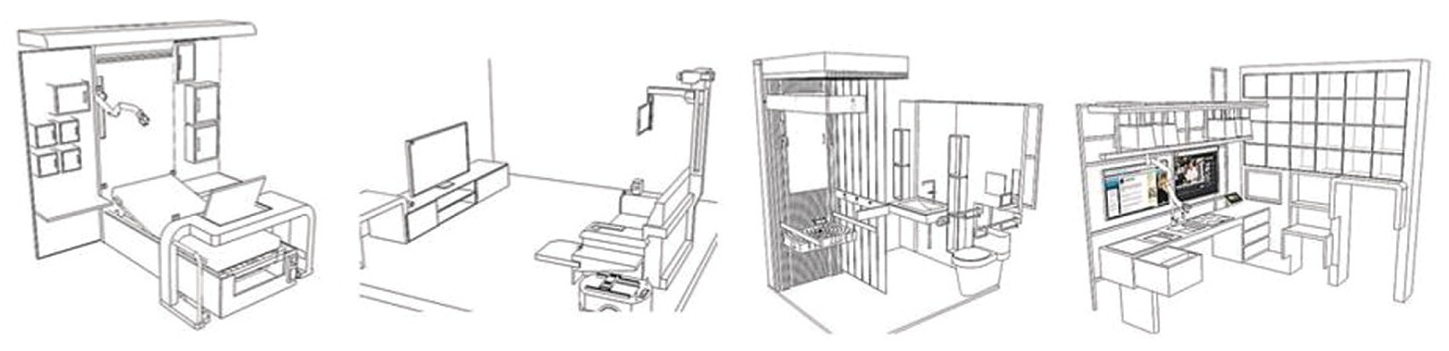
Figure 5.42 Subsystem 4: examples of Personalized Interior Intelligent Units (PI²U).
REACH also deals with the optimization of the products architecture and the management of PI²U’s complexity through modularity which can be considered a key factor for achieving replicability, mass-production, as well as customization of the PI²Us.